11.10 Inspection of the Precordium
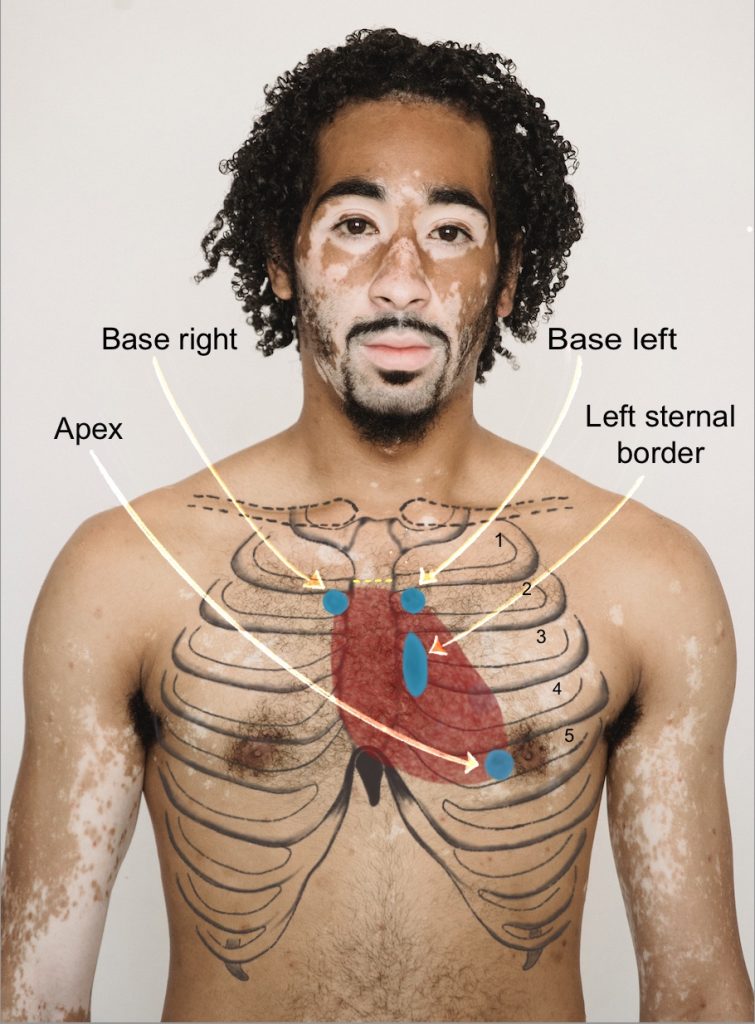
The precordium is the region on the chest wall that overlays the heart area. The base of the heart is located in the region of the second intercostal space and the apex is located in the region of the fifth intercostal space on the left side. As you inspect the chest wall, you will collect data that provides information about cardiac function.
Inspection of Precordium
Step 1: Place the client in supine position with their head on a pillow.
Step 2: Provide draping.
Step 3: Use tangential lighting with a penlight across the heart area.
Step 4: Inspect the base of the heart, left sternal border, and apex of heart. You may do this in sequence so that you are only exposing the area that you are assessing and then move on to the next area. See Figure 11.6 and Video 6.
Step 5: Inspect the skin over the precordium for any abnormal color changes. Normal skin should be uniform in color. Note any signs of cyanosis (bluish tint), erythema (redness), or pallor, which could indicate underlying cardiac conditions.
Step 6: Observe for the presence or absence of impulses against the chest wall and note the location.
- Pulsations: These are gentle flickers observed on the skin of the chest wall. They can be considered normal when observed on clients with thin chest walls. Otherwise, these are cues that require further assessment because they may be suggestive of increased cardiac workload associated with conditions such as an enlarged heart.
- Heaves: These are a more forceful movement (a thrust) observed on the skin over the chest wall. These cues require further assessment because they also may be suggestive of increased cardiac workload such as an enlarged heart.
-
In most individuals, the apical impulse is not visible upon routine inspection unless the person has a lean body type or increased cardiac output. It is typically felt rather than seen during a physical examination. If the apical impulse is visibly pronounced, it may suggest cardiac enlargement or other underlying conditions, warranting further clinical evaluation.
Step 7: Note the findings.
- Normal findings might be documented as: “Precordium inspected, skin color uniform with no abnormalities such as cyanosis, erythema, or pallor. No visible discolorations or irregularities detected. No cardiac impulses observed against chest wall.”
- Abnormal findings might be documented as (example): “Observed a slight, uniform pink discoloration across the precordium, consistent with patient’s baseline skin tone variations. No associated symptoms or distress reported; no clinical concern at this time. Gentle pulsation observed at apex.” or “Heave observed at apex.”
Video 6: Inspection of precordium.
Knowledge Bites: Pathophysiology
Impulses observed on the chest wall should always be assessed further because they are suggestive of some sort of increased workload of the heart and/or vasculature (such as the aorta). A heave can be associated with cardiac hypertrophy (enlargement of the heart muscle) or a dissecting aorta (a tear in the inner arterial wall that can lead to a rupturing of the aorta). These can be caused by many conditions such as hypertension, valvular disease, septal defects, and infarction. Your assessment can contribute to the database about whether the impulse is benign, such as may appear with a client who has a thin chest wall, or whether the impulse may have a pathophysiological cause.
