Chapter 2 – Other Models for Promoting Community Health and Development
Section 2-1: Healthy Cities/Healthy Communities
-
WHAT IS HEALTHY CITIES/HEALTHY COMMUNITIES?
-
WHY USE HEALTHY CITIES/HEALTHY COMMUNITIES?
-
WHO SHOULD PARTICIPATE IN HEALTHY CITIES/HEALTHY COMMUNITIES?
-
HOW DO YOU USE HEALTHY CITIES/HEALTHY COMMUNITIES?

In this video, Tyler Norris, Vice President of Kaiser Permanente Center for Total Health, discusses the meaning and impacts of community health. “What is a healthy community? What is healthy, and what is a community?” He asks. In this section, we will explore the concepts of defining, creating, and promoting healthy communities.
WHAT IS HEALTHY CITIES/HEALTHY COMMUNITIES?
Healthy Cities/Healthy Communities is a theoretical framework for a participatory process by which citizens can create healthy communities. In 1985, at a conference in Toronto organized by Trevor Hancock, Len Duhl spoke about his long-held conviction that health issues could only be effectively addressed through an inclusive, community-wide approach. Ilona Kickbusch, a World Health Organization (WHO) official who was attending the conference, brought the idea back to her superiors at the WHO European office in Copenhagen. Within a matter of weeks, Duhl and Hancock had been hired as consultants to help WHO and Kickbusch start a Healthy Cities movement in Europe. A year later, the attendees of a WHO conference in Ottawa drafted the Ottawa Charter, the “Constitution” of Healthy Cities/Healthy Communities. In the years since that first conference, the concept has spread to hundreds of large and medium-sized cities on all continents, and has also been used in smaller municipalities and rural communities in both the developing and the developed world. It is now the standard way in which the WHO addresses community health, and it encompasses other community issues as well.
A healthy community, as we discussed above, is one in which all systems work well (and work together), and in which all citizens enjoy a good quality of life. This means that the health of the community is affected by the social determinants of health and development – the factors that influence individual and community health and development.
So, what does the Healthy Cities/Healthy Communities model look like? Unlike PRECEDE/PROCEED, it has no flow chart or diagram, largely because its process may be totally different in different communities.It’s a loosely-defined strategy that asks citizens and officials to make becoming a healthy community a priority, and to pursue that end by involving all community members in identifying and addressing the issues most important to them.
We have created an informal logic model in order to connect you to your Community Tool Box resources that can support your effort to implement Healthy Cities/Healthy Communities.
Healthy Cities/Healthy Communities rests on two basic premises:
A comprehensive view of health. As we’ve been discussing, a comprehensive view of health takes in all the elements of a community’s life, since they affect both individual health and the health of the community itself. The Ottawa Charter lays out the prerequisites for health in communities:
Peace. This can be interpreted to cover both freedom from warfare, and freedom from fear of physical harm.
During the Vietnam War, young black men on the streets of their home neighborhoods in the U.S. were statistically more likely to be killed by gunfire than were young black soldiers in combat. Those home neighborhoods weren’t at peace, by anyone’s definition.
Shelter. Shelter adequate to the climate, to the needs of the occupants, and to withstand extremes of weather.
Education. Education for children (and often adults as well, as in the case of adult literacy) that is free, adequate to equip them for a productive and comfortable life in their society, and available and accessible to all.
Food. Not just food, but enough of it, and of adequate nutritional value, to assure continued health and vigor for adults, and proper development for children.
Income. Employment that provides an income adequate for a reasonable quality of life, and public support for those who are unable to work or find jobs.
A stable ecosystem. Clean air, clean water, and protection of the natural environment.
Sustainable resources. These might include water, farmland, minerals, industrial resources, power sources (sun, wind, water, biomass), plants, animals, etc.
Social justice. Where there is social justice, no one is mistreated or exploited by those more powerful. No one is discriminated against. No one suffers needlessly because she’s poor or ill or disabled. All are treated equally and fairly under the law, and everyone has a voice in how the community and the society are run.
Equity. Equity is not exactly the same thing as equality. It doesn’t mean that everyone gets the same things, but that everyone gets, or has access to, what he needs.
If all of these factors are considered, then health must extend far beyond medical treatment to all aspects of community life.
A commitment to health promotion. Health promotion differs from the more familiar medical models of treatment and prevention. Both of these look at health from a negative point of view: there’s something wrong or potentially wrong, and the medical expert will step in to fix it or head it off. Health promotion looks at it from a positive point of view: you can take positive steps to improve and sustain your well-being.
Health promotion – and we’ll use the term here to mean the promotion of healthy communities as well as healthy individuals – is a key both to the thinking behind the Healthy Cities/Healthy Communities concept, and to actually developing healthy communities. It calls for a commitment on the part of all sectors of the community, particularly government, to promote community health by:
Building healthy public policy. Communities can establish policies that foster the health of the community. According to the Ottawa Charter, such policies are “coordinated action that leads to health, income, and social policies that foster greater equity.” Thus, smoking bans in restaurants, local tax policies that encourage businesses to create jobs, training for police and youth workers to help them communicate with youth and curb youth violence, and strong environmental ordinances might all be seen as healthy public policy. Community support of such policy produces an atmosphere that makes it easier for policy makers to make the right choices, because they know the public is behind them.
Like all elements of a Healthy Cities/Healthy Communities strategy, healthy public policy is about a great deal more than simply fostering individual health – it’s about public policy that fosters a healthy society. That means equity, health for all, and attention to such things as supportive environments (see below).
Len Duhl talks about the fact that most public policy doesn’t deal with real needs, but rather with concerns of economics and power. For public policy to be healthy, it has to reflect reality, rather than what policy makers want to see, or what will get them elected. Objectivity leads to public policy that benefits everyone, not just the influential few.
Creating supportive environments. Community environments run the gamut from the physical to the social to the economic to the political. Some supportive environments can be created by laws or regulations, some by community effort, and some only by changes in attitude (which may or may not be influenced by social and other pressures). Some examples:
The natural environment. Laws and regulations that restore and/or preserve clean air and water; preservation and creation of open space, natural beauty, and wilderness; restrictions on the use and disposal of toxic substances; conservation of natural resources, including plants and animals. All of these can enhance health and reduce stress, provide an aesthetic experience, and affect community life for the better.
The Peak to Peak Healthy Communities Project, based in Nederland, CO, is working on renovating parks and creating a transportation link from downtown to trails and natural areas outside the city.
The built environment. People-friendly design of buildings and spaces (human scale, with pedestrian passageways, gathering places, views, attractiveness, etc.); handicap access; preservation of historic and cultural heritage; cleanliness; safety (lighting, building and bridge design, long views, traffic patterns, bans on the use of toxic materials); good public transportation; traffic-free paths to encourage walking, jogging, and bicycling.
For example, a city that builds or designates traffic-free walking and bike paths will probably see more of its citizens walk and bicycle to work and on errands than one where walking and biking are difficult and dangerous. Davis, California, for instance, has encouraged bicycling since 1960, when it became the first city in the US to paint bike lanes on its streets. It has been able to discontinue its school bus service, because it’s so easy for children to bike, walk, or skate to school on its miles of car-free bike paths.
The economic environment. A healthy economic environment is one where there is work for everyone capable of working, where workers are treated as assets (see directly below) and are paid a living wage, where there is equal economic opportunity for all, where those who can’t work are supported, and where money doesn’t buy political power or immunity from the law.
Bethel New Life, a faith-based, grass roots initiative in the Garfield Park neighborhood of Chicago, started out to rehabilitate derelict housing in the area, using “sweat equity” – i.e., the labor of local residents, who could then exchange their work for part of the cost of the home they had rebuilt. Now, Bethel employs more than 300, mostly local residents, in housing, employment training and job placement, economic development, cultural, family support, and community development programs. Its board is drawn almost wholly from the community, and its programs are responses to voiced community need. Bethel continues to try to build assets and bring greater economic stability to the West Side of Chicago.
The work environment. The work environment should be a source of stimulation, rather than stress. Respect for employees, good safety precautions and procedures, firm rules forbidding harassment or abuse, adequate pay and/or other compensation, humane and fair production expectations and treatment – all contribute to work environments that nurture creativity and enthusiasm, and improve, rather than detract from, both production and workers’ quality of life.
The leisure environment. The work and home environments can provide time for leisure. The community can provide recreational and cultural opportunities to use in that leisure time: museums, parks and beaches, cultural and sports events, libraries, etc.
The social environment. A healthy community encourages social networks, provides gathering places where people from all parts of the community may mingle, nurtures families and children, offers universal education and other services, strives to forster non-violent an healthy behavior, invites familiartity and interaction among the various groups that make up the community, and treats all groups and individuals with respect.
The North Quabbin Community Coalition, in north central Massachusetts, was concerned, among other things, with the high incidence of child physical and sexual abuse in the area. A task force on the issue eventually developed into Valuing Our Children, a parent education and family life program, that has trained large numbers of area parents as “parent educators,” and that provides services to area families.
The political environment. In a healthy community, all citizens have a say in how and by whom their community is governed, and have easy access to the information necessary to understand political situations and to make informed political decisions. Political decisions, opinions, and speech are protected. Citizens feel they have the power in the community – that they own it, and can and should control its direction.
Strengthening community action. Communities can encourage and strengthen community action in at least three ways: The first involves encouraging and fostering grass roots planning and action. When issues are identified and addressed by the people affected by them, as well as by others concerned, two things happen: the issues are more likely to be resolved successfully, and the people involved learn how to use their own resources to take charge of their lives and their communities. A second way of strengthening community action is through a commitment from government, community leaders, and other decision makers to encourage action by passing legislation conducive to it, lending public support to it through the media and other communication channels, and including members of all segments of the community in the conception, planning, and implementation of any community initiative. The third is by decision makers and the media ensuring a free and accurate flow of necessary information about the community and community initiatives to all citizens, and providing everyone in the community with learning opportunities about issues and about the quality of life in general.
The latter two of these methods are really top-down conceptions where government and others in power “let” citizens share in the decision-making process. While community members – particularly those with less experience in planning and running projects, or with less education – often need support to learn some necessary skills, the drive for change can and should come from them to begin with. There is a big difference between officials organizing an initiative and inviting citizens to join, and officials approaching citizens with a request to participate in envisioning and organizing an initiative.
Developing personal skills. Healthy communities aid their citizens in gaining the skills necessary to address health and community issues, by providing education and information in school, home (through the media and other sources), work, and community settings. Courses, workshops, billboards and posters, TV and radio ads, newspaper articles, mailings, fliers, community meetings, presentations in social clubs and churches, the use of electronic technology – all might serve to help citizens understand an issue, and make decisions about it.
The education referred to here doesn’t relate only to health and wellness issues and life skills (e.g., parenting). In fact, it could, and does, apply to all learning that touches on topics related to the life of the community – political, social, environmental, and economic issues, for instance. Furthermore, the encouragement and accessibility of lifelong learning is a mark of a healthy community.
Reorienting services. To be useful to a Healthy Cities/Healthy Communities strategy, health and other human and municipal services have to change from an individual- and treatment-centered point of view to one that is community-centered and focuses on the promotion of a healthy community.
It’s not only a matter of reorienting health services, but one of reorienting all services to work together toward the goal of a healthy community. Any community issue has to be viewed through the lenses of both the individual and the community. It takes a village not only to raise a child, but to pull families out of poverty, to create employment, to improve mental health, to stop violence, to safeguard the natural environment, and to create a just and equitable society.
WHY USE HEALTHY CITIES/HEALTHY COMMUNITIES?
There are a number of reasons to consider using the Healthy Cities/Healthy Communities framework in planning and implementing community action:
- Community perspective. Virtually all health and community issues are affected by (or are the direct result of) economic, social, political, and/or environmental factors that operate at the community level. If you don’t deal with those factors, the chances are slim that you’ll be able to resolve the issue you’re concerned with.
- Participatory planning and community ownership. Planning that includes those who will be directly affected by or benefit from any community initiative is more likely to reflect the real needs of the community than planning done only by one group. Furthermore, the participatory nature of the Healthy Cities/Healthy Communities framework means that citizens themselves create initiatives and goals for the community. Those initiatives and goals are theirs – not imposed by those in power or by outside “experts”. As a result, their commitment to the process and to the goals makes them far more likely to support and work for the outcomes they’ve chosen.
- Range of ideas. Citizen participation leads to the presentation and consideration of a greater range of ideas and possibilities, and is therefore more likely to hit upon effective goals and actions.
- Knowledge of the community. Citizen participation taps the community’s wisdom about its own history, relationships, and conflicts, and can thus steer initiatives around potentially fatal pitfalls.
- Community-wide ties. Involving all segments of the community encourages interaction across social, economic, and political lines. Those ties strengthen the community as a whole, change people’s perspectives for the better, increase community-wide cooperation, and can positively transform how the community works.
- Achievable and measurable goals. Although Healthy Cities/Healthy Communities’ ultimate goals are wide and long-term, each goal is achievable in a manageable amount of time, and its successful achievement can be demonstrated. Each success sets the stage for enthusiasm for the next initiative.
- Identification and use of community assets and resources. A Healthy Cities/Healthy Communities initiative depends to a large extent on human, institutional, organizational, environmental, and other assets and resources already available within the community. Through identifying and using these, communities learn that they can create their own positive change, and reshape themselves in the ways they want to.
- Community commitment to the long-term process. Because of the participatory nature of the process, and because it requires recruiting more people at each new phase, it builds an ever-expanding core of people with varied skills, talents, and experience committed to the ideal of building a healthy community and improving the quality of life for everyone. That’s important for sustaining the work indefinitely.
- Community self-image. Through the use of the Healthy Cities/Healthy Communities process, the community comes to think of itself as a healthy community, and is concerned with maintaining that image through addressing issues as they come up. Perhaps more important, it is brought to look at the larger picture as well. Holding out an ultimate goal of a totally healthy community, whether attainable or not, keeps everyone working toward it, and means that planning goes on as a matter of course. The healthy community ideal becomes embedded in the self-image of the community, and people understand that they can take their fate in their own hands and work to improve it. The process itself thus becomes an important element in the definition of a healthy community – one in which citizens work together to identify and solve problems, create and consolidate assets, generate improvements, and raise the quality of life for all.
WHO SHOULD PARTICIPATE IN HEALTHY CITIES/HEALTHY COMMUNITIES?
The easy answer to this question is everyone in the community, and that’s in fact the ideal. In a perfect world, everyone everywhere would participate in some way in creating a healthy community. In the real world, while it’s important to try to involve all sectors of the community, you have to work to involve some particular people and groups if your effort is to be successful. Crucial participants include:
- Elected and appointed officials. Although a Healthy Cities/Healthy Communities initiative should not be top-down, it needs the commitment and backing of those with the power to make things happen. Officials can use the media to publicize the effort, pass laws and regulations (and enforce those already existing) that reinforce it, and throw the weight and resources of government behind it. Without official support, a community-wide effort is more likely to fail.
- Those most affected by the issue. A sure recipe for failure is to try to impose an intervention or initiative on a population “for their own good.” All too often, “experts” – often people who have no real knowledge of the group or its issues – formulate plans that might make perfect sense on paper, but make no sense at all in the actual situation for which they’re proposed. The participation of those affected in identifying the issues to address, developing action plans for addressing them, and implementing and overseeing those plans is absolutely crucial to the success of a Healthy Communities initiative. (This is equally true when the group concerned is the whole community.)
There are, unfortunately, many instances of a group resisting and short-circuiting well-meaning changes because they weren’t part of the planning. The author experienced one as a teacher in Philadelphia, which had, at the time, an innovative and progressive school superintendent. He tried to institute reforms that probably would have improved the lives of teachers students in the system, but he did it without conferring with them. As a result, the teachers simply ignored directives from the central office, the reforms failed, and the superintendent was gone within three years.
- The people who will actually administer and carry out the initiative, or whose jobs or lives will be affected by it. It is both unfair and unwise to expect organization staff, community employees (police, firefighters, Department of Public Works personnel, etc.), business people, and others to throw themselves into carrying out an initiative they had no part in devising. It may have elements that ignore the realities of their jobs or their lives, or that make things harder than necessary for them, and they may be the only people who have the information to understand that. In addition, they may regard it as just another foolish imposition to be gotten around, and do as little as possible to make it effective.
- All the agencies and groups that will need to cooperate and to coordinate their activities in order to implement a community-wide effort. Both the ways in which these groups will work together, and which of them will have responsibility for what have to be part of the planning for any community-wide initiative. Without their full participation, there’s no guarantee that they’ll work together at all, let alone that the methods for their doing so will be simple and efficient.
- Community opinion leaders. These are the people whose opinions others trust, and who lead the community by adopting new ideas and pulling others with them. They are seen as level-headed, smart, and serving the best interests of the community. Some may be current or former members of the groups already listed, and others may be clergy, credible institutional or business people (college presidents or faculty, CEO’s), or just average citizens who are known for their integrity and common sense.
If you can gain the participation of members of all these groups, it is more likely that everyone else will follow. If you can’t get people from all these groups to buy in at the outset, an alternative is educating them about the process and persuading them to join it, while you continue to recruit other participants. Ultimately, the combination of education and your momentum will bring in those who were initially reluctant. That may take time and patience, but it’s worth the effort – it can easily mean the difference between a successful long-term Healthy Community movement and a dead-on-arrival, failed attempt at one.
HOW DO YOU USE HEALTHY CITIES/HEALTHY COMMUNITIES?
Because the Healthy Cities/Healthy Communities framework is just that – an intellectual framework, rather than a prescription – there is no step-by-step instruction for employing it. It is meant to be adapted to the different needs of different communities. There are, however, necessary components of any Healthy Cities/Healthy Communities initiative:
- Create a compelling vision based on shared values. As with virtually any process that involves planning – and particularly participatory planning – the first step is to create a vision that defines the effort to be made. That vision may be broad (“A community that is truly just and equitable”) or more specific (“A community where every potential worker in the community can find employment that offers a living wage and acceptable working conditions”). Whatever the case, the vision must be compelling – one that motivates people to work for its realization. It must be founded in those values that they hold in common, and must be widely shared and recognized as legitimate and desirable.( Proclaiming Your Dream: Developing Vision and Mission Statements.)
In Orlando, Florida, the Healthy Community Initiative began with meetings of a few influential people. As they learned about healthy communities, the convened a group of about 160, representing all sectors of the city’s population – citizens of all races and economic levels, organizations and institutions, city government, other groups – to hash out a vision. That group, in turn, conducted citizen focus groups and public meetings to hear and understand citizens’ concerns. Ultimately, they drafted a vision, based on their own discussions and the input of hundreds of others from all walks of life, that contained 14 statements about what Orlando should be. That vision became the foundation of the initiative.
- Embrace a broad definition of health and well-being. Health must be seen as not merely the physical health of individuals, but the creation and nurturing of those factors leading to health named in the Ottawa Charter (peace, shelter, education, income, food, a stable ecosystem, sustainable resources, social justice, and equity). A truly healthy community encompasses – or works toward – all those elements and more.
- Address quality of life for everyone. The key word here is “everyone.” A Healthy Cities/Healthy Communities initiative should be aimed at improving the quality of life for all groups and individuals in the community, not just those in a particular target group or those who began the initiative.
- Engage diverse citizen participation and be citizen-driven. Initiatives should be originated, planned, and implemented with the full participation of citizens from all racial, ethnic, and socio-economic groups and all walks of life. Citizens themselves, rather than a government agency or experts of some sort, should be the force behind both the direction and the implementation of any community initiative.
- Seek multi-sectoral membership and widespread community ownership. All sectors of the community – government, the business and non-profit communities, health care, education, faith communities, cultural institutions and the arts, target populations, and ordinary citizens – should be represented in an initiative, and the community should feel that it created the initiative and owns it.
In many places in this and other sections of the Community Tool Box, we refer to “ownership” of an initiative or intervention or organization. In most cases, what we mean is that those who take part in creating and/or running such an endeavor feel that it belongs to them. It was their idea, and they therefore see themselves as not only supportive of it, but responsible for it.
True ownership can rarely, if ever, be attached to actions or ideas that are imposed, by others who “know better” or have more power. It comes from within, from the feeling that you’ve made a choice based on your best judgment. That’s why the inclusion of people from all sectors of the community is so important to a successful Healthy Cities/ Healthy Communities process. At the end, perhaps after a lot of argument and soul-searching, participants feel that they’ve had a hand in creating something important that will result in better lives for everyone in the community. There’s no substitute for that feeling to ensure their doing all they can to make their creation work.
- Acknowledge the social determinants of health and the interrelationship of health with other issues (housing, education, peace, equity, social justice). The research on the social determinants of health points to three overarching factors:
- Socioeconomic equity. For developed countries, the economic and social equality within the society or a given community is a greater determinant of death rates and average lifespan than the country’s position with regard to others. The size of the income gap between the most and least affluent segments of the society or community is tremendously important, and determines to a large extent whether people get what they need.
- Social connectedness. Many studies indicate that “belonging” – whether to a large extended family, a network of friends, a social or volunteer organization, or a faith community – is related to longer life and better health, as well as to community participation.
- Sense of personal efficacy. This refers to people’s sense of control over their lives. People with a higher sense of efficacy tend to live longer, maintain better health, and participate more vigorously in community affairs and politics.
Like the Ottawa Charter, the World Health Organization, in its publication The Solid Facts, recognizes the need to break these factors down into more manageable pieces. It lists ten factors that affect health and life expectancy, and advocates addressing each within a coherent program that looks at all of them within a society. These ten factors are:
- The social gradient (equity)
- Stress
- Early life
- Social exclusion (the opposite of social connectedness)
- Work
- Unemployment
- Social support
- Addiction
- Food
- Transport
- Address issues through collaborative problem-solving. Given a diverse group, there are bound to be disagreements and conflicts. These should be viewed as opportunities, rather than roadblocks, and people should be encouraged and helped to work together to reach creative solutions.
- Focus on systems change. To be successful, a Healthy Cities/Healthy Communities initiative has to be active, rather than reactive. It’s not enough to “fix” a problem: your goal is to eliminate the causes of that and other problems and improve the long-term quality of life in the community in the process.
In order to address causes, you have to concentrate not on individual problems, but on improving and changing systems – the ways in which the community operates, and the attitudes, assumptions, and policies behind them. That includes identifying, using, and strengthening the assets the community already possesses, as well as changing the systems that pose problem
- Build capacity using local assets and resources. All communities, no matter how troubled, have great real and potential strengths. These vary from community to community, but could include:
Individuals with the talents, skills, leadership, and passion to work to change the community for the better.
Individuals, businesses, and foundations that can provide material resources – money, space, etc. – to a community effort.
- Institutions – libraries, schools, hospitals, houses of worship – that have the capacity to act as both resources for and agents of change.
- Community-based and other organizations whose mission is to work for the betterment of the whole community.
- Governments and individual government officials that can add both official support and legal and regulatory power to an initiative.
- Human resources – the skills and work ethic of the community’s work force, for example.
- Natural and other environmental resources – open space, clean air and water, wilderness, fisheries, historic sites or buildings, housing stock.
- Perhaps most important, the potential for all these individuals, groups, and resources to be joined in a coordinated pursuit of a common vision.
- At least some of these and other assets already exist in virtually every community – usually to a far greater extent than most citizens realize until they start looking for them. They must be identified and included in a Healthy Cities/Healthy Communities effort.
- Measure and benchmark progress and outcomes. Whatever you’re doing, whether it’s a PR campaign or a complex behavioral intervention, you have to monitor and evaluate it in order to be sure that it’s effective. That means setting objectives – benchmarks – to indicate your progress along the road to your goal, and defining clearly the outcome you’re aiming for. Regularly monitoring what you’re doing is crucial, because it allows you to spot problems or inadequacies in goals, methods, procedures, communication, etc. and correct them before they derail your initiative entirely. Even more important, regular monitoring allows you to change what you’re doing to respond to changes in circumstances and community needs, so that you’re always addressing current reality. Communities are dynamic: they develop and change, sometimes in short periods. Your initiative has to be dynamic, too, especially if you expect it to continue for the long term.
IMPLEMENTING A HEALTHY COMMUNITIES STRATEGY
How do you actually put these components together to create a healthy community? There’s no one way to do that – it depends on your community, the issues you want to address, and the ideas and capacities of the groups and individuals that participate in the Healthy Cities/Healthy Communities process. There are, however, some basic procedures that, at least in outline, should be common to any Healthy Cities/Healthy Communities initiative.
- Assemble a diverse and inclusive group. To begin a Healthy Cities/Healthy Communities initiative, people from all parts of the community have to come together to hammer out a vision. That group, as we’ve been saying throughout this section, should be representative of everyone in the community, so that whatever it decides will be seen as legitimate by just about everyone, and will be owned by the community.
Someone has to start the process. That may be a charismatic or persistent individual, an organization, a coalition, or a government office or agency. Whoever it is should be simply a convener, and not necessarily expect to lead over the long term. Leaders should be chosen by the group itself as it forms, and they should be collaborative ( Collaborative Leadership.)
This is not to say that a Healthy Communities effort doesn’t need leadership. Quite the contrary – leadership and structure are necessary for any successful effort. But leadership should be collaborative and arise from the community. The leader may be an individual, or two, or a larger group. Whatever the situation, the leadership should be one of an equal among equals, and decision-making should be the province of the whole group. That’s how a participatory process works.
It is assumed that all the other steps listed here will also be carried out by an inclusive group, and that all sectors of the community – including those affected and individual citizens – will be represented and have decision-making power. The group may change from step to step or over time, but should remain inclusive and participatory.
- Generate a vision. A vision of how the community should be, based not on a single issue, but on values shared among all participants and on a high quality of life for everyone in the community, is needed to motivate and inspire participants and to guide the initiative over the long term. Generating such a vision may take time and a great deal of discussion, but it’s absolutely necessary for a successful effort.
- Assess the assets and resources in the community that can help you realize your vision, and the issues that act as barriers to it. Placing assets first is not just an accident here. A Healthy Cities/Healthy Communities initiative is best served by looking at the community through a positive lens, and asking first what’s right with it, rather than what’s wrong with it. The initiative then becomes an exercise in community health promotion, instead of the treatment of a diseased community. Taking a positive perspective affects for the better the attitudes of everyone involved, the community’s self-image, and the perception of whether or not realizing your vision is possible. By the same token, it’s important to be honest and clear-eyed about issues and problems in the community. Once they’ve been identified, they have to be acknowledged and understood, so they can be addressed at some point in the process.
- Choose a first issue to focus on. The best way to sink a long-term initiative is to try to accomplish all your goals at once. It’s vital to choose one issue – or in some cases, perhaps, two or three – to attack, and to make it one that can be resolved, so that your first effort leads to success.
What the issue is doesn’t matter, except in that it must be one chosen by citizens as important to them, and must be one that is specific enough to be resolvable. Len Duhl talks about the process in a 1993 interview by Joe Flower in Healthcare Forum Journal.
The first thing that happens when the Healthy Cities program develops in a new place is that some persons assume the responsibility of bringing together all segments of the community to deal with the issues: the business community, the government, the voluntary sector and the citizens themselves. …
Then there are “vision workshops” in which people are asked, “What kind of city do you really want?” My personal surprise is that the clearer I am about what a Healthy City program is, the less likely a community is to develop it. The fuzzier I am in what a Healthy City is, “A Healthy City is what you want to make it,” the greater the odds are that they will start.
The various participants define the program. All I say is that you have to start someplace. You have to begin to look at it in an ecological and systemic way. You have to involve people. You have to start thinking of values of equity and participation. Beyond that, you can start wherever you want.
Some cities start on the environment, on pollution, on smoking, seat belts and the quality of life index. Some have government operations, some have newspapers, big organizations, housing. Barcelona linked it to the Olympics. Glasgow linked it to developing itself as the cultural capital of Europe. It is being done every way.
- Develop a community-wide strategy, incorporating as many organizations, levels, and sectors as possible. Here’s where Healthy Cities/Healthy Communities differs most from many logic models and other methods that are clear on exactly how to go about planning and carrying out an initiative. Rather than offering a step-by-step process, HC might use any participatory planning process that incorporates a community-wide approach and that looks at all the possible areas that might affect the issue chosen. Thus, you might use VMOSA, PRECEDE/PROCEED, or some variant, or a less structured process – whatever seems appropriate and works for your community.
It is important, however, that your plan result in a community-wide, multi-pronged approach. If your focus is on youth violence, for instance, it should involve some sort of action or supportive function by local government, parents and parent advocates, schools, law enforcement, the court system, welfare, agencies that deal with youth and families, physical and mental health services, Family Planning, the media, adult literacy (dropouts), and potentially or formerly violent youth and their victims. All of these groups and individuals should be working together as a team, each referring youth to other appropriate services or agencies among them, and all coordinated and collaborating in their operation. The focus should be on changing the systems that make a problem possible, or that present barriers to the ideal the community is working toward.
- Implement the plan. Once again, this should involve a community-wide effort. Any oversight of the implementation should include a broad range of individuals and groups, representing a cross-section of the community.
- Monitor and adjust your initiative or intervention. Once you’ve implemented your plan, it’s crucial to evaluate the effectiveness of both your process (Are you doing what you set out to do?) and your results (Are you reaching your benchmarks? Are you having the planned effect on the issue?) If an evaluation gives unsatisfactory answers to any of these questions, you can revisit the issue, determine the reasons your plan isn’t working well, and change it accordingly.
- Establish new systems that will maintain and build on the gains you’ve made. Once you’ve reduced youth violence, for example, you still have to do whatever is necessary to make sure it doesn’t rise again, and that it continues to decline. (What’s the ultimate goal here? Is there an acceptable level of youth violence?) That may mean setting up new organizations or programs, working to change or cement changes in community attitudes and procedures, redesigning school curricula, working regularly with the media – whatever it takes to sustain progress.
- Celebrate benchmarks and successes. Public celebration of achievements not only energizes those who have been working toward them, but informs the community that the drive toward a healthy community is moving forward successfully. It helps to establish the idea of a healthy community in the public mind, and to build a foundation for the continuation of the initiative.
- Tackle the next issue(s). The ultimate goal here is the development of a truly healthy community, which translates to improving the quality of life for everyone in the community. After your first success, it’s time to use your momentum to address another (or more than one other) issue. That may be the removal of a barrier to a healthy community, or it may be the creation of a necessary element of a healthy community. In either case, it means sustaining citizens’ commitment to an ongoing and long-term process, the end result of which is a community controlled by its residents, where all systems work toward the public good.
IN SUMMARY
The health of a community, like that of an individual, depends on far more than freedom from pain or disease. Health, or its lack, for a community is the result of a large number of factors, often intertwined, that span the social, economic, political, physical, and environmental spheres. Virtually any community issue has an effect on, and is affected by, the overall health of the community as a whole, and therefore should be approached in a community context. Healthy Cities/Healthy Communities provides a philosophical framework for an inclusive, participatory process aimed at raising the quality of life for everyone, and creating a truly healthy community.
Two basic premises underlying the Healthy Cities/Healthy Communities concept are a comprehensive view of health and community issues, covering a broad range of factors that contribute to a healthy community; and a commitment to the active promotion of a healthy community, rather than the “treatment” of problems. By addressing the social and other determinants of health and community issues (including the Ottawa Charter’s list of peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice, and equity), and by creating appropriate policy and environments, encouraging social action, providing personal skills, and reorienting services to a more wide-ranging approach, communities can foster citizen empowerment and equity.
REASONS FOR ADOPTING THE HEALTHY CITIES/HEALTHY COMMUNITIES APPROACH INCLUDE:
- Its community perspective, leading to a more effective approach to issues.
- Community ownership of any effort, resulting from community participation in its development and implementation.
- The broad range of ideas gained from a participatory process.
- Its access to citizens’ knowledge of the community, helping to avoid pitfalls caused by ignorance of community history and relationships.
- The forging of community-wide and ties that cross economic, social, racial, and other lines.
- Participatory planning leading to solutions that reflect the community’s real needs.
- The adoption of achievable goals, leading to success.
- The identification and use of community assets and resources which both take advantage of what already exists, and teach the community what it can do with its own considerable resources.
- The fostering of community commitment to the process of building a healthy community.
- The creation of a healthy community self-image.
While a Healthy Cities/Healthy Communities process should involve everyone, some particularly important participants include local government and officials; those affected by the issue(s); those who will actually administer and implement the initiative, or whose lives or jobs will be affected by it; any organizations that will be expected to work together; and opinion leaders.
There are 10 important components of a Healthy Cities/Healthy Communities process:
- Create a compelling vision based on shared values.
- Embrace a broad definition of health and well-being.
- Address quality of life for everyone.
- Engage diverse citizen participation and be citizen-driven.
- Multi-sectoral membership and widespread community ownership.
- Acknowledge the social determinants of health and the interrelationship of health with other issues (housing, education, peace, equity, social justice).
- Address issues through collaborative problem-solving.
- Focus on systems change.
- Build capacity using local assets and resources.
- Measure and benchmark progress and outcomes.
Although there is no one step-by-step procedure for a Healthy Cities/Healthy Communities initiative – both the content and the structure of the process depend upon your community’s needs, and, particularly on community decisions – there is, given the ten components above, a reasonable way to approach it in most cases.
- Assemble a diverse and inclusive group.
- Generate a vision.
- Assess the assets and resources in the community that can help you realize your vision, and the issues that act as barriers to it.
- Choose a first issue to focus on.
- Develop a community-wide strategy, incorporating as many organizations, levels, and sectors as possible.
- Implement the plan.
- Monitor and adjust your initiative or intervention.
- Establish new systems that will maintain and build on the gains you’ve made.
- Celebrate benchmarks and successes.
- Tackle the next issue.
PowerPoint: 2.7_0
Online Resources
(The goal in choosing sites here has been to offer a few that give background or general information on Healthy Cities/Healthy Communities, and a few that are the sites of specific programs. Nearly every Healthy Cities site seems to have its own web page, and these can easily be found by searching “healthy cities” and/or “healthy communities.”)
Bethel New Life, a grass roots, church-based urban development effort in the Garfield Park neighborhood of Chicago. A bottom-up initiative that grew organically over many years, responding to the voiced needs of the community. Most staff and board members are community residents.
Mesa County, CO: A case study of community transformation. A grass roots effort that involved the whole community and grew into the Civic Forum; and a more top-down community health assessment.
Community Partners, Inc., an organization deeply involved in the Healthy Communities movement.
Essential State Level Capacities for Support of Local Healthy Communities Efforts, by Peter Lee, Tom Wolff, Joan Twiss, Robin Wilcox, Christine Lyman, and Cathy O’Connor.
Greater Orlando Healthy Communities Initiative. A very top-down effort, started by current and former Junior League presidents, the newspaper editor, the mayor, and other prominent citizens. They involved the community with the help of a consultant.
The Healthy Communities Program in Aiken, South Carolina. A “model” program, focused on infant mortality. A top-down effort, it nonetheless involves the community in planning and input, and has been highly successful not only at reducing infant mortality, but at providing other needed services, many not directly related to health.
Healthy Cities information from WHO Denmark, the godfather of the Healthy Cities/Healthy Communities movement.
The Healthy Cities initiative of Illawarra, Australia.
Healthy People in Healthy Communities, a guide from the US Dept. of Health and Human Services.
The International Healthy Cities Foundation.
Links to numerous articles on Healthy Cities/Healthy Communities from the Change Project. Includes interviews with Len Duhl and Ilona Kickbusch by Joe Flower from the Healthcare Forum Journal.
The Ottawa Charter.
The Peak to Peak Healthy Communities Project, Gilpin County, Colorado.
The Twenty-Fifth Anniversary of Healthy Communities
WHO information on Healthy Cities
Print Resources
Norris, T. (2002). America’s Best Kept Secret: The Healthy Communities Movement. (Reprint by Healthy Communities Massachusetts from the National Civic Review, introduction, Spring, 1997.) Pan American Health Organization. Healthy Municipalities and Communities: Mayors’ Guide for Promoting Quality of Life. Washington, DC.
Public Health, Vol. 115, Nos. 2 and 3 (March/April & May/June, 2000): Focus on Healthy Communities., Vol. 115.
Wilkinson, R., & Michael M. (1998) eds. The Solid Facts: Social Determinants of Health. World Health Organization: Copenhagen.
Section 2-2: Ten Essential Public Health Services
Before you read this section’s information about the Ten Essential Services, we invite you to take a quiz. Answers are provided at the bottom of this page. See how well YOU do!
(1).As you read the front page of the local paper, you notice an alarming article about an outbreak of “disease X” in your community. You read on to learn about the scientifically established cause of “disease X”, and precautionary measures for avoiding exposure.
This valuable information was published as a front-page story because:
a. The local football team lost its game last night
b. The front-page columnist is on vacation
c. State and local health officials and their staff have worked for weeks to gather data, conduct laboratory and statistical tests, generate hypotheses, and collaborate with the media to alert and educate the public about “disease X” as effectively as possible.
(2).On your way into the local grocery store, you notice a flier advertising a toll-free hotline number for enrolling uninsured children in a federally funded health insurance program.
This insurance program is being offered because:
a. The federal government has a budget surplus and is looking for a way to spend it
b. A leading telephone company offered the state health department a great deal on 1-800 numbers
c. Public health professionals have documented the numbers of uninsured children in their states, and worked with federal and state policymakers to institute outreach and “wrap around services” that assure the universal provision of health care.
(3).While shopping in the local mall, you come across a group of nurses offering free blood pressure and cholesterol screenings.
The nurses are offering these screenings because:
a. They need to moonlight
b. They enjoy people watching at the mall
c. They are public health nurses dedicated to community health promotion, including the prevention of heart disease
(4).You and your sweetheart share a romantic dinner at your favorite restaurant. Not only is the meal delicious – you do not get food poisoning!
This enjoyable experience has been brought to you by:
a. The restaurant management
b. Your local health department
c. A joint effort of the restaurant management and your local health department
(5).In an urban area, prevalent liquor stores are slowly being replaced by grocery stores. The mass transit system has been re-routed to guarantee store access to urban residents without vehicles.
This change in the community’s planning and development is probably a result of:
a. The Department of Transportation needing to increase revenue
b. The liquor storeowners deciding that they weren’t doing enough business and moving elsewhere.
c. A collaborative effort of citizens, public health professionals, city planners, and local government officials who share the common goal of preventing substance use and alcoholism among members of their urban community.
(Answers: 1. c; 2. c; 3. c; 4. c; 5. c)
What, besides the same answer, do the quiz scenarios above have in common? They are real life, everyday examples of some of the Ten Essential Public Health Services that public health professionals strive to deliver in the counties and states that they serve.
This Tool Box section will teach you what the Ten Essential Public Health Services are, and illustrate the function of those Services in public health. When you have completed the tool, you will be able to identify under which Essential Service public health activities in your community are implemented. More importantly, we hope that you will understand how the synergy of efforts within all ten Essential Service areas can contribute to the health of your community’s populations.
To help you get started with identifying how the Ten Essential Public Health Services are reflected in day-to-day public health activities, Table 1 below matches five of the Ten Essential Public Health Services with their corresponding quiz scenarios.
Table 1: Examples of How Essential Services Are Reflected in Day-to-Day Public Health Activities
|
Quiz Scenario
|
Essential Public Health Service Implemented
|
|
Informing the public about an epidemiological outbreak investigation in the community
|
“Investigate, diagnose, and address health hazards and root causes”
|
|
Promoting enrollment in a federally subsidized health insurance program
|
“Enable equitable access”
|
|
Health education and health promotion to prevent heart disease
|
“Communicate effectively to inform and educate”
|
|
Maintenance of a sanitary restaurant environment for public well-being
|
“Utilize legal and regulatory actions”
|
|
Shaping health policy, city planning, and transportation routes to create an environment that fosters positive health behavior
|
“Create, champion, and implement policies, plans, and laws”
|
We hope that you want to read on and learn more. But before we discuss each of the Essential Services, we will visit the broader concept of defining the purpose and function of public health.
WHAT IS PUBLIC HEALTH?
As you probably concluded from the quiz scenarios, public health is everywhere – it is a part of the infrastructure that keeps our communities safe and healthy.
Depending on which resource you read, you will find varying definitions of the mission of public health. However, the most current and widely accepted mission definition is:
“Promote physical and mental health, and prevent disease, injury, and disability.”
Public health services may go unnoticed within a community because they are often (but not always) preventive versus reactive. For example, which community service are you more likely to notice – an environmental health specialist inspecting the safety of a local university’s food service establishments, or a fire truck speeding down the street with its lights and sirens on?
Despite having a relatively ‘low profile’ status, public health services play a key role in assuring the health and well being of communities. Throughout the 1900s, the average lifespan of persons in the United States increased by more than 30 years. According to an article by Bunker, Frazier, and Mosteller (1994), 25 years of this are attributable to advances in public health.
WHO IS THE TYPICAL PUBLIC HEALTH PROFESSIONAL?
There really is no “typical” public health professional. The public health workforce in the United States consists of approximately 500,000 individuals with diverse professional training and experience.
- Some are nurses, physicians, or laboratory technicians by training.
- Some are educators, nutritionists, or social workers by training.
- Some are biostatisticians or epidemiologists.
- Others are economists or lawyers.
- Community-based or “grassroots” workers might include concerned parents, grandparents, or civic leaders who volunteer their time.
How do all of these people with a unified purpose but different skills work together successfully to carry out the mission of public health? They have a logic model to consult: the Ten Essential Services of Public Health.
The Ten Essential Services of Public Health differ in some ways from other logic models presented in Chapter 2 of the Tool Box. Other logic models discussed incorporate prescribed processes (e.g., from planning to implementation to evaluation) diagrammed in a flow chart that can then be applied to one priority goal like teen pregnancy prevention. In contrast, there is no prescribed order of implementation for the Ten Essential Services—no flow chart, and no one specific outcome that results from implementing all ten Essential Services. Rather, the Ten Essential Services have the potential to create a comprehensive infrastructure that can provide a supportive context for any public health priority in a community.
Although the more prescriptive logic models may be narrow in scope once applied to one goal, they can also undertake a comprehensive approach within a community. For example, a planning phase might involve stakeholders from non-public health sectors of the community, in an effort to foster the most supportive context for change. This is not unlike the impact of the Ten Essential Services.
You may be wondering,
“Why do people need a logic model for direction if they are already working towards the same mission?”
Because of their diverse backgrounds, some professionals have been trained to follow different paradigms (models) in their specialties. One example is the “medical model” versus the “public health model.” The most significant difference between the two models is that public health activities focus on entire populations, while clinical activities focus on individual patients. Table 2 below summarizes key differences between the paradigms that are typically used to train clinical and public health professionals.
Table 2: Public Health versus Medical Models of Professional Training
|
Public Health Model |
Medical Model |
| Primary focus on population | Primary focus on the individual |
| Public service ethic, tempered by concerns for the individual | Personal service ethic, conditioned by awareness of social responsibilities |
| Emphasis on prevention and health promotion for the whole community | Emphasis on diagnosis, treatment, and care for the whole patient |
| Paradigm employs a spectrum of interventions aimed at the environment, human behavior and lifestyle, and medical care | Paradigm places predominant emphasis on medical care |
The Ten Essential Public Health Services provide a common ground for professionals trained in either paradigm, as well as grassroots workers and non-public health civic leaders, so they can work collaboratively towards fulfilling the public health mission:
“To promote physical and mental health, and prevent disease, injury, and disability.”
Now that you have a better understanding of public health, let’s talk about the origin, purpose, and function of the Ten Essential Public Health Services.
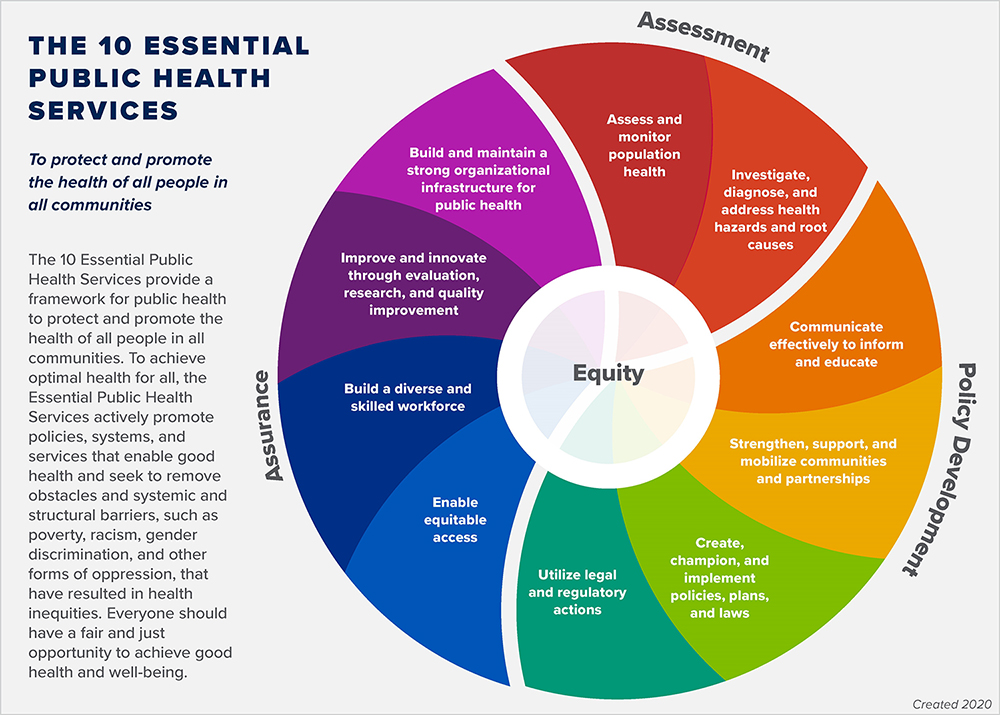
WHAT ARE THE TEN ESSENTIAL PUBLIC HEALTH SERVICES?
From 1988 to the early 1990s, the recognized “core functions” of public health were:
- Assessment
- Policy development
- Assurance
In 1993, with a new presidential administration and federal and state attempts to reform the health care system in the United States, public health leaders decided to set forth a more detailed and utilitarian consensus statement that would “speak with one voice” to public health professionals, the general population, and the policymakers who would shape health care reform.
Public health leaders worked to define a more detailed logic model of core public health functions. The end result was a consensus statement that included the Ten Essential Public Health Services, adopted in 1994.
WHY IS IT IMPORTANT TO IMPLEMENT AND MONITOR THE TEN ESSENTIAL PUBLIC HEALTH SERVICES?
- The Ten Essential Public Health Services are really about actualizing the public health paradigm that we presented in Table 2. Let’s review the key principles involved:
- A primary focus on the population
- A public service ethic, tempered by concerns for the individual
- An emphasis on prevention and health promotion for the whole community
- The paradigm employs a spectrum of interventions aimed at the environment, human behavior and lifestyle, and medical care
The theme of prevention is the most powerful element in the implementation of the Ten Essential Public Health Services.
- Through prevention, countless injuries, illnesses, and even chronic diseases can be avoided.
- Through prevention, lives can be saved.
- Through prevention, health care cost can be contained.
- Through prevention, individuals, their families, and their communities can benefit from the population-based reach of the Ten Essential Public Health Services.
It is important to not only implement but also monitor—or track, assess, and modify, as needed—the Ten Essential Public Health Services. With data or other information about the Services’ costs or expenditures, implementation, and impact, monitoring can contribute to informed policy decisions about public health program development and funding at local, state, and national levels.
HOW ARE THE TEN ESSENTIAL SERVICES USED IN COMMUNITY PRACTICE?
On the pages that follow, each Essential Service is discussed in order from 1 to 10. Each discussion includes a definition of the Service and some examples of national or community practice. Keep in mind that the Services do not necessarily need to be implemented in the “1 – 10” sequence, or even independently.
The Ten Essential Services are independent yet complementary goals for communities to work toward. You should actually strive to implement the services simultaneously in your community as a means of carrying out the mission of public health. However, you may find that you identify with only one or two in terms of your role in your community’s public health initiatives as you read through this section.
Essential Service #1: Assess and monitor population health.
Public health surveillance—the ongoing, systematic collection, analysis, and interpretation of health related data—is at the core of this Essential Service.
Essential Service #1 encompasses public health activities such as:
- Identification of threats to health and assessment of health service needs;
- Timely collection, analysis, and publication of information on access, utilization, costs, and outcomes of personal health services;
- Attention to the vital statistics and health status of specific groups that are at higher risk than the total population; and
- Collaboration to manage integrated information systems with private providers and health benefit plans.
National level, population-based surveillance systems administered by the Centers for Disease Control and Prevention (CDC) include:
- The Behavioral Risk Factor Surveillance System;
- National Vital Statistics System;
- National Health Interview Survey; and
- Cancer registries;
You can access CDC data electronically at the Centers for Disease Control and Prevention website. You may not immediately think to use national level data when working at the community level. However, national level surveillance data can provide trend data to use as a benchmark as you assess health status measures (e.g., the number of children immunized prior to entering preschool) in your community. Prior to investing resources and time in a program, it is often necessary to conduct a needs assessment. Community data collected via a needs assessment can be compared to existing data at the national level. If you discover that your community actually has an excellent rate for a health status measure as compared to 75% of the states in the country, you may shift your prevention program priorities to a different measure or target population!
If you do not have the time or resources to conduct your own needs assessment, you can search for community level data in resources including:
- State-level ‘report cards’ on maternal and child health indicators (see the federal Title V Information System with data for all U.S. states and territories).
- School health reports; and
- Law enforcement agency surveillance, such as the number of DUI arrests
Essential Service #2: Investigate, diagnose, and address health hazards and root causes.
Essential Service #2 encompasses public health activities such as:
- Epidemiologic identification of emerging health threats;
- Public health laboratory capability using modern technology to conduct rapid screening and high volume testing;
- Active infectious disease epidemiology programs; and
- Technical capacity for epidemiologic investigation of disease outbreaks and patterns of chronic disease and injury.
At the national level, the United States Department of Health and Human Services oversees the Agency for Toxic Substances and Disease Registry (ATSDR). The Agency’s overall function is to “serve the public by using the best science, taking responsive public health actions, and providing trusted health information to prevent harmful exposures and disease related to toxic substances.”
Via grants and cooperative agreements, ATSDR provides funding and technical assistance for states to identify and evaluate environmental health threats to communities, as well as educate the communities about health risk or other findings.
At the local level, public health laboratories provide diagnostic testing, disease surveillance, applied research, laboratory training and other essential services to the communities they serve. Laboratory work is diverse, yet accomplished by highly trained and skilled professionals.
Public health laboratory professionals and epidemiologists are the ones working behind the scenes on the issues that you hear about in the news. These include: newborn screening; Lyme disease; West Nile virus; food borne illness outbreak investigations; and bio-terrorism threats. The Association of Public Health Laboratories was founded by state and territorial public health laboratory directors serving communities across the United States. You may want to visit this website to learn more about the public health laboratory expertise and services available in your own community.
Essential Service #3: Communicate effectively to inform and educate.
You have probably come across—and even participated in— health promotion and social marketing efforts in your community.
Essential Service #3 encompasses public health activities such as:
- Social marketing and targeted media public communication (e.g., Toll-free information lines);
- Providing accessible health information resources at community levels (e.g., free, mobile health screening initiatives);
- Active collaboration with personal health care providers to reinforce health promotion messages and programs; and
- Joint health education programs with schools, churches, and worksites (e.g., stress reduction seminars; parenting support groups for enhancing mental health; and health fairs).
You may have noticed national media campaign advertisements on television, billboards, or even posters or fliers in your doctor’s office. Some examples include the “Back to Sleep” campaign to prevent Sudden Infant Death Syndrome, or the anti-substance use campaign, “Just Say No.”
Many national awareness weeks also relate directly to public health efforts. The American Public Health Association, headquartered in Washington, D.C., actually sponsors a “National Public Health Week” each spring. You can find additional information, and links to free tools and resources for National Public Health Week. You may decide to sponsor an event such as a fun run or health fair to raise public health awareness in your own community!
Essential Service #4: Strengthen, support, and mobilize communities and partnerships.
These activities represent a comprehensive approach to community health, in which professionals and even entire sectors of a community collaborate to plan, implement, monitor, evaluate, and subsequently modify activities, and repeat the process as needed.
Essential Service #4 encompasses public health activities such as:
- Convening and facilitating community groups and associations, including those not typically considered to be health-related, to undertake defined preventive, screening, rehabilitation, and support programs; and
- Skilled coalition-building ability in order to draw upon the full range of potential human and material resources in the cause of community health.
This is not unlike the PATCH logic model – the Planned Approach to Community Health
Included in the PATCH strategy are five elements that are fundamental to the success of any community health promotion process:
- Community members participate in the process.
- Data guide the development of programs.
- Participants develop a comprehensive health promotion strategy.
- Evaluation emphasizes feedback and program improvement.
- The community capacity for health promotion is increased.
You can read about a similar process for mobilizing community partnerships to identify and solve health problems in the Community Tool Box’s Community Action Guide: A Framework for Addressing Community Goals and Problems.
The overall goal of action planning is to increase your community’s ability to work together to affect conditions and outcomes that matter to its residents—and to do so both over time and across issues of interest.
As your community works towards a broad vision of health for all, creating supportive conditions for change requires comprehensive efforts among diverse sectors of the community. These include health organizations, faith communities, schools, and businesses. Representatives of each sector come together to form a community coalition. Your community coalition can strive to influence systems changes—programs, policies, and practices that can enhance or detract from the community’s capacity to be a supportive environment for healthy living.
Essential Service #5: Create, champion, and implement policies, plans, and laws.
Because state and local public health programs are often funded at least in part with Federal dollars, accountability is often a key issue. Public health programs therefore document progress towards positive change in health behavior or health status indicators. For example, the Federal Maternal and Child Health Services Block Grant, which imposes a $3 state match for every $4, requires annual reporting of “performance measures.” Some of those are state-negotiated to allow for flexibility in tracking health behavior or health status indicators that are unique to a state’s populations. Data such as these can be presented to policymakers to document the value or effectiveness of a program. Those data can also be used for continued program planning and modification.
Essential Service #5 encompasses public health activities such as:
- Leadership development at all levels of public health;
- Systematic community-level and state-level planning for health improvement in all jurisdictions;
- Development and tracking of measurable health objectives as a part of continuous quality improvement strategies;
- Joint evaluation with the medical health care system to define consistent policy regarding prevention and treatment services; and
- Development of codes, regulations, and legislation to guide the practice of public health.
Active Living by Design is a national program of The Robert Wood Johnson Foundation, and is a part of the University of North Carolina at Chapel Hill School of Public Health. The program establishes and evaluates innovative approaches to increase physical activity through community design, public policies, and communications strategies. The program funds community partnerships to develop, implement and sustain collaboration among a variety of organizations in public health and other disciplines, such as city planning, transportation, architecture, recreation, crime prevention, traffic safety and education, and key advocacy groups. Collaborators focus on land use, public transit, non-motorized travel, public spaces, parks, trails, and architectural practices that advance physical activity.
One example of an Active Living by Design initiative is: “Obesity and The Built Environment: Improving Public Health through Community Design.” You can learn more about this and other initiatives by visiting Active Living by Design.
Essential Service #6: Utilize legal and regulatory actions.
While you may not always be conscious of how public health regulations have influenced your community environment, think about some of the things that you see or experience when you visit restaurants. You may have noticed a framed certificate hanging on the wall, with “Sanitation Grade A.” This certificate is a result of local health department inspections to assure that the restaurant is in compliance with food storage, handling, and preparation regulations.
While at that same restaurant, you may also notice a sign that says, “No smoking.” This may be a direct result of a statewide law that was designed to improve the environmental health conditions in your community.
If you have school-aged children and have had to prepare them for entrance into the public school system, you know that the full series of immunizations is required. Immunizations are required for school-aged children in the United States because when widespread immunizations are in place, we all benefit from what is referred to as “herd immunity.” When a group of people (e.g., an entire community, state, or nation) is immunized against an infectious disease, it makes it more difficult for the disease to spread and cause an epidemic.
Essential Service #6 encompasses public health activities such as:
- Full enforcement of sanitary codes, especially in the food industry;
- Full protection of drinking water supplies;
- Enforcement of clean air standards;
- Timely follow-up of hazards, preventable injuries, and exposure-related diseases identified in occupational and community settings;
- Monitoring quality of medical services (e.g., laboratory, nursing homes, and home health care); and
- Timely review of new drug, biologic, and medical device application.
Essential Service #6 may be implemented in your community as a result of either state or federal legislation. Not only can you take on a leadership role in your community to assure that public health regulations are enforced; you can be a catalyst for change by identifying and prioritizing new issues, and sponsoring new regulations through public health advocacy.
Essential Service #7: Enable equitable access.
Essential Service #7 encompasses public health activities such as:
- Assuring effective entry for socially disadvantaged people into a coordinated system of clinical care;
- Culturally and linguistically appropriate materials and staff to assure linkage to services for special population groups;
- Ongoing “care management;”
- Transportation services;
- Targeted health information to high risk population groups; and
- Technical assistance for effective worksite health promotion/disease prevention programs.
The implementation of this Essential Service is inherently linked to the social, economic, and political climate in communities, states, and the nation. To assure the provision of health care when it is otherwise unavailable, the United States federal government funds two “safety net” programs: Medicaid and the State Children’s Health Insurance Program (SCHIP).
Medicaid is the largest source of funding for medical and health-related services for people and families with low incomes and resources. This program became law in 1965, and is jointly funded by the federal and state governments (including the District of Columbia and the Territories) to assist states in providing medical long-term care assistance to people who meet certain eligibility criteria.
The Balanced Budget Act of 1997 created a new children’s health insurance program called the State Children’s Health Insurance Program (SCHIP). SCHIP is a state administered program, and each state sets its own guidelines regarding eligibility and services for children up to age 19 who are uninsured. Families who earn too much to qualify for Medicaid may still be able to qualify for SCHIP.
To learn more about the Medicaid and SCHIP programs and how they can benefit members of your community, please visit: Centers for Medicare and Medicaid Services.
The availability of programs like Medicaid and SCHIP is not sufficient. Public health professionals also have to provide outreach services to the populations in need of these programs. Outreach might include:
- Consumer education about the existence of a program;
- Assistance with applying for a program;
- Linking enrollees to related health programs (for example, pregnant women, infants, and children under the age of 5 enrolled in Medicaid also qualify for the Federal Supplemental Food Program for Women, Infants, and Children—WIC, and vice versa);
- Physically transporting clients to the medical services that they need.
Culturally and linguistically appropriate materials are a critical component of outreach efforts in a country in which many immigrant languages are spoken. Public health professionals can use decennial census data or community level needs assessments to determine how many and which languages are spoken in a geographic region. To provide outreach and other services in a culturally competent manner, public health professionals can apply guidelines developed by the National Center for Cultural Competence. The Center produces publications that teach people how to adapt health promotion materials already developed and written in English.
Essential Service #8: Build a diverse and skilled workforce.
Essential Service #8 encompasses public health activities such as:
- Education and training for personnel to meet the needs for public and personal health service;
- Efficient processes for licensure of professionals and certification of facilities with regular verification and inspection follow-up;
- Adoption of continuous quality improvement and life-long learning within all licensure and certification programs;
- Active partnerships with professional training programs to assure community-relevant learning experiences for all students; and
- Continuing education in management and leadership development programs for those charged with administrative / executive roles.
There are many opportunities for certified education, training, and continuing education in public health. The Association of Schools of Public Health is a membership organization of the 27 accredited schools of public health that prepare people for a public health profession. The accrediting body, an independent agency recognized by the United States Department of Education, is the Council on Education for Public Health.
Continuing education opportunities abound at professional conferences and in professional journals. Furthermore, the advent of the Internet has brought new access to continuing education through the availability of online certificate and other training programs. These distance-based programs—particularly the ones offered through accredited schools of public health—offer an invaluable alternative to the sometimes-prohibitive costs and time commitment of travel for state and local public health professionals.
The Centers for Disease Control and Prevention sponsors many training and continuing education opportunities on site and in the accredited schools of public health across the country. One example is Academic Centers for Public Health Preparedness (A-CPHP). These centers work together to improve the capacity of the front line public health and health care workers to quickly respond to bioterrorism, infectious disease outbreaks, and other public health threats and emergencies.The network of Centers represents a unique partnership between the schools of public health, the Association of Schools of Public Health, the Centers for Disease Control and Prevention, and representatives from state and local public health agencies, and the Association of State and Territorial Health Officials (ASTHO) and National Association of County and City Health Officials (NACCHO).
Other programs meet the education and training needs of rising public health professionals while simultaneously enhancing workforce capacity in the field. One example is the Federal Maternal and Child Health Bureau’s Graduate Student Internship Program, which places Maternal and Child Health graduate students in state health departments for summer internships via a competitive process for both health departments and students.
Essential Service #9: Improve and innovate through evaluation, research, and quality improvement.
Evaluation helps public health professionals continually refine or revise program approaches in future years of funding. Furthermore, evaluation data provide information about the relative costs and effort for tasks so activity and budget adjustments can be made.
Essential Service #9 encompasses public health activities such as:
- Ongoing evaluation of health programs based on analysis of health status and service utilization data, to assess program effectiveness and to provide information necessary for allocating resources and reshaping programs.
The process of evaluation helps public health professionals and their collaborators assess the success of community health initiatives. Evaluation normally requires that data be collected and analyzed. Surveillance data from Essential Service #1 can be used for this purpose. For example, because surveillance efforts are often (but not always) annual, your community could access retrospective and current or “baseline” data before planning a public health initiative.This baseline data could then also be used to document the health behavior or health status outcome measure(s) of interest both before and after implementation of the initiative.
Evaluation plans and concepts are addressed in several chapters and sections of the Community Tool Box. These include:
Chapter 36–39, all of which fall under the broad topic,“Evaluating Community Programs and Initiatives”
Essential Service #10: Build and maintain a strong organizational infrastructure for public health.
In order to implement the 10th Essential Service, state and local health department staff might carry out health services research via many different efforts including:
- Continuous linkage with appropriate institutes of higher learning and research;
- An internal capacity to mount timely epidemiologic (e.g., outbreak investigations) and economic analyses (e.g., cost-benefit studies); and
- An internal capacity to conduct needed health services research (e.g., survey design; conducting interviews and facilitating focus groups; conducting clinical trials; and accessing and using public records).
This list of research activities further illustrates the need for skills-specific training and education prescribed in Essential Service number 8. For example, anyone can create a survey and interview a group of people. However, there are prescribed methods for creating an “instrument” that collects information that can be summarized into a coherent and even statistically significant conclusion about a population of interest. Local health department staff may have had formal academic or on-the-job training in questionnaire design, survey methodology, or biostatistics. Some staff may even be “specialists” who can be called upon to complete complex data analyses for research purposes. However, both generalists and specialists in the local health departments contribute to the base of knowledge and experience that are critical to maintaining an internal capacity to conduct needed health services research.
Even when local health department staff have adequate training, a strain on staffing capacity or limited resources may prompt collaboration with other “specialists.” Within the public health community, it is not difficult to find examples of health departments working with neighboring universities to conduct research and identify solutions. One example is the Association of Schools of Public Health’s Academic Health Departments (AHD) grant program. The AHD program fosters collaboration among local health departments across the country and 14 neighboring universities that house accredited schools of public health. The exchange of student and other resources can enhance the capacity of local health agencies to function as “learning organizations,” thereby enhancing the success of community health efforts.
Another example of linkages with institutes of higher learning is the Council on Linkages Between Academia and Public Health Practice. Housed within the non-profit Public Health Foundation in Washington, D.C., the Council has a mission to “Improve public health practice and education by fostering, coordinating, and monitoring links between academia and the public health and healthcare community, developing and advancing innovative strategies to build and strengthen public health infrastructure, and creating a process for continuing public health education throughout one’s career.”
Research for new insights and innovative solutions to health problems can be accomplished many different ways. One way is via economic analyses to assess the “cost benefit” or the “cost effectiveness” of a program.
A cost-benefit evaluation assesses only one program, and focuses on the cost-to-outcome ratio, with the “outcome” having a dollar amount attached to it. Example: For a program that invests in prevention, the amount spent per client on prevention would be compared to the amount saved in averted health care costs per client (e.g., “For every $2 that we spend on diabetes management education, we save $4 in hospitalization costs.”).
A cost-effectiveness analysis can be used with one or multiple programs with the same objectives, to relate the cost of a program approach to specific measures of a program’s objectives. Those measures may or may not have a monetary value attached to them (e.g., an outcome measure for an education program may be standardized test scores).
Online Resources
- American Public Health Association
- Association of Schools of Public Health
- Association of State and Territorial Health Officials
- Environmental Council of the States
- Essential Public Health Services. Public Health Foundation (2002)
- The Essential Services of Public Health. American Public Health Association (2003)
- National Association of County and City Health Officials
- National Association of State Alcohol and Drug Abuse Directors
- National Association of State Mental Health Program Directors
- Programs in Brief Centers for Disease Control and Prevention (2003)
- Public Health Code of Ethics (Issue Brief) American Public Health Association
- Public Health Foundation
- Publich Health Quality Improvement Exchange (PHQIX) allows people to submit short explanations of their initiatives and observations/lessons-learned.
- United States Public Health Service
- What is Public Health? Association of Schools of Public Health (2003)
GUIDE FOR ENHANCING CORE FUNCTIONS AND ESSENTIAL SERVICES FOR PUBLIC HEALTH IMPROVEMENT
1. Assess and monitor population health.
- Analyzing Community Problems
- Assessing Community Needs and Resources
- Collecting Information About the Problem
- Conducting Concerns Surveys
- Conducting Focus Groups
- Conducting Interviews
- Conducting Needs Assessment Surveys
- Conducting Public Forums and Listening Sessions
- Conducting Surveys
- Determining Service Utilization
- Developing a Plan for Assessing Local Needs and Resources
- Developing Baseline Measures of Behavior
- Identifying Community Assets and Resources
- Understanding and Describing the Community
2. Investigate, diagnose, and address health hazards and root causes.
- Adapting Community Interventions for Different Cultures and Communities
- Analyzing Community Problems
- Analyzing Problems and Goals
- Analyzing Root Causes of Problems: The “But Why?” Technique
- Collecting Information About the Problem
- Conducting Interviews
- Defining and Analyzing the Problem
- Designing Community Interventions
- Developing an Intervention
- Ethical Issues in Community Interventions
- Identifying Targets and Agents of Change: Who Can Benefit and Who Can Help
- Identifying Strategies and Tactics for Reducing Risk
- An Introduction to the Problem Solving Process
- Understanding Risk and Protective Factors: Their Use in Selecting Potential Targets and Promising Strategies for Interventions
3. Communicate effectively to inform and educate.
- Arranging a Press Conference
- Arranging News and Features Stories
- Communicating Information about Community Health and Development Issues
- Creating Brochures
- Creating Fact Sheets on Local Issues
- Creating Newsletters
- Creating Posters and Fliers
- Creating a Website
- Conducting a Social marketing Campaign
- Developing a Plan for Communication
- Developing Creative Promotions
- Handling Crises in Communication
- Implementing a Social Marketing Effort
- Making Community Presentations
- Our Model of Practice: Building Capacity for Community and System Change
- Preparing Press Releases
- Preparing Guest Columns and Editorials
- Preparing Public Service Announcements
- Reframing the Issue
- Some Lessons Learned on Community Organization and Change
- Talking About Risk and Protective Factors Related to Community Issues
- Using Paid Advertising
- Using E-mail Lists
4. Strengthen, support, and mobilize communities and partnerships.
- Attracting Support for Specific Programs
- Changing Policies to Increase Funding for Community Health and Development Initiatives
- Community (Locality) Development
- Creating Objectives
- Developing an Action Plan
- Our Model of Practice: Building Capacity for Community and System Change
- Our Evaluation Model: Evaluating Comprehensive Community Initiatives
- Working Together for Healthier Communities: A Framework for Collaboration Among Community Partnerships, Support Organizations, and Funders
- Developing a Plan for Getting Community Health and Development Issues on the Local Agenda
- Developing an Ongoing Board of Directors
- Developing Strategic and Action Plans
- Developing Successful Strategies: Planning to Win
- Identifying Action Steps in Bringing About Community and System Change
- Maintaining a Board of Directors
- Marketing the Initiative to Secure Financial Support
- Obtaining Feedback from Constituents: What Changes Are Important and Feasible?
- Organizational Structure: An Overview
- An Overview of Strategic Planning or VMOSA (Vision, Mission, Objectives, Strategies, Action Plan)
- Proclaiming Your Dream: Developing Vision and Mission Statements
- Promoting Adoption of the Initiative’s Mission and Objectives
- Promoting Coordination, Cooperative Agreements, and Collaborative Agreements Among Agencies
- Social Action
- Sustaining the Work or Initiative
- Strategies for the Long-Term Institutionalization of an Initiative: An Overview
- Strategies for Sustaining the Initiative
- Welcoming and Training New Members to a Board of Directors
5. Create, champion, and implement policies, plans, and laws.
- Advocating for a Change
- Conducting a Petition Drive
- Conducting a Public Hearing
- Developing a Plan for Advocacy
- Encouraging Involvement of Potential Opponents as well as Allies
- Filing a Complaint
- General Rules for Organizing for Legislative Advocacy
- Identifying Opponents
- Lobbying Decisionmakers
- Overview: Getting an Advocacy Campaign Off the Ground
- Recognizing Allies
- Survival Skills for Advocates
- Understanding the Issue
- Using Personal Testimony
- Writing Letters to Elected Officials
- Writing Letters to the Editor
6. Utilize legal and regulatory actions.
- Adapting Community Interventions for Different Cultures and Communities
- Building Leadership
- Capturing What People Say: Tips for Recording a Meeting
- Coalition Building I: Starting a Coalition
- Conducting Effective Meetings
- Creating and Maintaining Coalitions and Partnerships
- Developing a Plan for Building Leadership
- Developing a Plan for Involving Volunteers
- Strategies for Community Change and Improvement: An Overview
- Social Action
- Using Principles of Persuasion
- Designing Community Interventions
- Developing a Community Leadership Corps: A Model for Service-Learning
- Developing a Plan for Increasing Participation in Community Action
- Developing Facilitation Skills
- Developing Training Programs for Volunteers
- Developing Volunteer Orientation Programs
- Establishing Micro-grant Programs
- Ethical Issues in Community Interventions
- Identifying Strategies and Tactics for Reducing Risks
- Identifying Targets and Agents of Change: Who Can Benefit and Who Can Help
- Involving Key Influentials in the Initiative
- Involving People Most Affected by the Problem
- Making Personal Contact with Potential Participants
- Methods of Contacting Potential Participants
- Promoting Neighborhood Action
- Promoting Participation Among Diverse Groups
- Recruiting Volunteers
- Servant Leadership: Accepting and Maintaining the Call of Service
- Training for Conflict Resolution
- Understanding Risk and Protective Factors: Their Use in Selecting Potential Targets and Promising Strategies for Interventions
- Writing Letters to Potential Participants
7. Enable equitable access.
- Developing Multisector Collaborations
- Identifying Opponents
- Increasing Participation and Membership
- Overview: Getting an Advocacy Campaign Off the Ground
- Promoting Coordination, Cooperative Agreements, and Collaborative Agreements Among Agencies
- Recognizing Allies
- Survival Skills for Advocates
- Understanding and Describing the Community
- Understanding the Issue
- Applying for Grants
8. Build a diverse and skilled workforce.
- Building Leadership
- Building and Sustaining Commitment
- Building and Sustaining Relationships
- Building Relationships with People from Different Cultures
- Capturing What People Say: Tips for Recording a Meeting
- Conducting a Workshop
- Conducting Effective Meetings
- Collecting Information About the Problem
- Conducting Needs Assessment Surveys
- Conducting Surveys
- Designing a Training Session
- Delivering a Training Session
- Defining and Analyzing the Problem
- Developing a Community Leadership Corps: A Model for Service-Learning
- Developing and Communicating a Vision
- Developing a Management Plan
- Developing a Plan for Staff Hiring and Training
- Developing a Plan for Building Leadership
- Developing Facilitation Skills
- Discovering and Creating Possibilities
- Enhancing Cultural Competence
- Generating and Choosing Solutions
- Healing from the Effects of Internalized Oppression
- Influencing People
- An Introduction to the Problem Solving Process
- Learning From and Contributing to Constituents
- Learning How to Be a Community Leader
- Making Decisions
- Multicultural Collaboration
- Promoting Coordination, Cooperative Agreements, and Collaborative Agreements Among Agencies
- Providing Supervision for Staff and Volunteers
- Providing Support for Staff and Volunteers
- Putting Your Solutions into Practice
- Servant Leadership: Accepting and Maintaining the Call of Service
- Transforming Conflicts in Diverse Communities
- Understanding Culture and Diversity in Building Communities
- Understanding People’s Needs
9. Improve and innovate through evaluation, research, and quality improvement.
- Behavioral Surveys
- Choosing Evaluators
- Communicating Information to Funders for Support and Accountability
- Conducting Interviews with Key Participants to Analyze Critical Events
- Constituent Survey of Outcomes: Ratings of Importance
- Developing an Evaluation Plan
- Establishing Formal Communication and Requesting Participation
- Evaluating the Initiative
- A Framework for Program Evaluation: A Gateway to Tools
- Gathering Data on Public Opinion
- Gathering Information: Monitoring Your Progress
- Gathering and Using Community-Level Indicators
- How to Conduct Research: An Overview
- Measuring Success: Evaluating Comprehensive Community Initiative
- Our Evaluation Model: Evaluating Comprehensive Community Initiatives
- Providing Feedback to Improve the Initiative
- Rating Community Goals
- Rating Member Satisfaction
- Reaching Your Goals: The Goal Attainment Report
- Understanding Community Leadership, Evaluators, and Funders: What Are Their Interests?
10. Build and maintain a strong organizational infrastructure for public health.
- Adapting Community Interventions for Different Cultures and Communities
- Assessing Community Needs and Resources
- Conducting Public Forums and Listening Sessions
- Collecting Information About the Problem
- Designing Community Interventions
- Developing a Plan for Assessing Local Needs and Resources
- Developing Multisector Collaborations
- Identifying Targets and Agents of Change: Who Can Benefit and Who Can Help
- Identifying Strategies and Tactics for Reducing Risks
- Understanding and Describing the Community
- Understanding Risk and Protective Factors: Their Use in Selecting Potential Targets and Promising Strategies for Interventions
- Promoting Coordination, Cooperative Agreements, and Collaborative Agreements Among Agencies
PowerPoint: 2.7_0
Print Resources
American Public Health Association (June 2003). The Guide to Implementing Model Standards. This resource includes discussion of PATCH implementation along with other model standards for community health development, such as the Assessment Protocol for Excellence in Public Health.
Association of Schools of Public Health (2003). The Population Approach to Public Health.
Centers for Disease Control and Prevention (1999). Ten Great Public Health Achievements—United States, 1900 – 1999. Morbidity and Mortality Weekly Report, April 02, 1999: 48(12); 241-243.
The remaining nine links will take you to the web pages of organizations that served on the Public Health Functions Steering Committee, which adopted the Ten Essential Public Health Services in 1994.
United States Department of Health and Human Services (1989). Making Health Communication Programs Work: A Planner’s Guide. Bethesda, MD: United States Department of Health and Human Services, Public Health Service, National Institutes of Health, Office of Cancer Communications, National Cancer Institute.
Wholey, J., Hatry, H., & Newcomer, K. (Eds.) (1994). Handbook of Practical Program Evaluation. San Francisco: Jossey-Bass.
Section 2-3: Some Lessons Learned on Community Organization and Change
Learn from those who have come together to address issues and bring about community-level improvements.

WHAT IS COMMUNITY ORGANIZATION?
Community organization is the process of people coming together to address issues that matter to them. Community members developing plans for how the city can be a place where all its children do well. Neighbors joining in protests to stop drugs and violence in their community. Members of faith communities working together to build affordable housing. These are all examples of community organization efforts.
WHAT ARE THE TYPES OF COMMUNITIES THAT ORGANIZE?
Community organization can happen in the variety of contexts that define “community.”
SHARED PLACE
People come together who share a common geographic place such as a neighborhood, city, or town. For example, local residents might come together to address neighborhood concerns such as safety, housing, or basic services. Problem solving through community-based organizations (CBOs), neighborhood associations, and tenants — organizations are common forms of place-based practice.
SHARED EXPERIENCE
Community organizing also occurs among people who share an experience, such as a shared workplace or shared experience with disabilities or health disparities. Those who share a common identity may organize around issues, such as discrimination, that are barriers to achieving common goals.
SHARED INTEREST
Organizing frequently occurs among those who have concerns about the same issues such as jobs, housing, child well-being, or education.
WHAT ARE SOME MODELS OF PRACTICE IN COMMUNITY ORGANIZATION?
Should community organization be about collaboration among people sharing common interests or confrontation with those in power? This is a false dichotomy that ignores the context of the work. Several models of practice emerged in various contexts of community organization work (Rothman, 1995).
SOCIAL PLANNING
Social planning uses information and analysis to address substantive community issues such as education, child development, or environmental health. For example, planning councils or task forces engage (usually) professionals in setting goals and objectives, coordinating efforts, and reviewing goal attainment.
Social planning might occur in a context of either consensus or conflict about goals and means. For example, information about high rates of adolescent pregnancy, and factors that contribute to it, may help communities focus on the goal of preventing teen pregnancy, and even decisions about using controversial means such as sexuality education and enhanced access to contraceptives. Use of social planning helps build agreement on common results.
SOCIAL ACTION
Social action involves efforts to increase the power and resources of low-income or relatively powerless or marginalized people. For example, advocacy organizations, such as those for disability rights or tobacco control, often use social action approaches. They might arrange disruptive events — including lawsuits, sit-ins, or boycotts — to draw attention and focus to their concerns by those in power.
Organizers create events, such as a protest or strike, that those in positions of power (such as employers) can avoid or stop by coming to an agreement. For example, people with disabilities might stop picketing a business when it modifies policies that discriminate against people with disabilities. Or, a tobacco company might avoid a lawsuit by tobacco control advocates by eliminating advertising directed at minors. Social action tactics are used in lots of situations involving conflicting interests and imbalance in power; they usually take place when conventional negotiations aren’t working.
LOCALITY DEVELOPMENT
Locality development is another way to get people to work together. It is the process of reaching group consensus about common concerns and collaborating in problem solving. For example, local residents in urban neighborhoods or rural communities may cooperate in defining local issues, such as access to job opportunities or better education, and in taking action to address the concerns.
COMMUNITY PARTNERSHIPS OR COALITIONS
There are many hybrid models that combine elements of the three approaches. For example, community partnerships or coalitions combine elements of social planning and locality development when people who share common concerns, such as child well -being or substance use, come together to address them. The goal of many coalitions is to change community conditions — specific programs, policies, and practices — that protect against or reduce risk for these concerns. These models, and their variations, may be implemented at local, state, regional, and even broader levels.
WHAT ARE SOME LESSONS LEARNED ABOUT COMMUNITY ORGANIZATION AND CHANGE?
The following summaries come from lessons learned from various experiences with community organization practice. The lessons are organized by broad topics related to the work of community organization and change.
The lessons come through experience within:
- Understanding (and affecting) community context
- Community planning
- Community action and mobilization
- Understanding (and addressing) opposition and resistance
- Intervention and maintenance of efforts
- Promoting community change
- Influencing systems (or broader) change
- Achieving community-level improvements
UNDERSTANDING (AND AFFECTING) COMMUNITY CONTEXT
High profile commissions and reports create conditions for experimentation and optimism about public problem solving.
For example, during the 1960s, the U.S. President’s Commission on Juvenile Delinquency helped spawn innovative efforts such as those of Mobilization for Youth in New York City. Similarly, in the early 1990s, a national level task force on infant mortality helped launch a multi-site demonstration program known as Healthy Start. High-profile studies such as this help set the public agenda by highlighting what should be addressed and how. Prominent reports frame the dominant explanations for societal problems. For example, a report could focus attention on poverty as a “root cause” of many societal problems or infant mortality as a pressing issue. It might also feature a promising alternative solution, such as equal access to health care or legal assistance, as an innovative way to address social problems.
You might need to use more than one model of community organization practice to fit the variety of contexts in which community work is done.
For example, social planning or locality development strategies may fit a context of consensus about common purpose such as working together to reduce violence. By contrast, the strategy of social action, with its disruptive activity and related conflict, may be more appropriate in a context of conflicting interests, such as organizing for decent wages or safe conditions in the workplace.
Crosscutting issues are good contexts for community organization practice.
Some community issues, for example, neighborhood safety or substance use, affect the majority of people who share a common place. They also offer a solid basis around which a critical mass of local people can work together. When community organization efforts involve people from diverse backgrounds of income and power — such as educational or public health improvements that affect people across social class — substantive change is a lot more likely to happen.
Community organization can’t always be separated from politics or controversy.
Consider the case of people coming together in a rural community to address issues of toxic waste and environmental pollution. Public debate may focus on both the economic interests of affected businesses, and the health concerns of local residents. It’s typical that when two parties are on opposite sides of an issue, neither will get everything they want. Inevitably, a resolution is going to involve politics: the art of reconciling or balancing competing interests.
Poor people can make substantial gains (or losses) during periods of tumultuous change, and related realignment of political parties.
Would there have been a Civil Rights Act of 1964 without rioting and a realignment of the Democratic Party? Political parties want to avoid mass protest or any unorganized behavior if it’s at all possible, by changing (or appearing to change) policies, programs, and practices related to voiced concerns. Since mass protest is something those in power try to avoid, it’s an important means by which poor people — with otherwise limited resources — can achieve power and influence.
Strategies used in community organization should match the times.
In times of turmoil, organizing protests and strikes by the people affected by the issues can yield maximum gains. By contrast, in the long times between periods of disruptive actions, community organization might use less conflict-oriented approaches, such as locality development or collaborative partnerships, to define and pursue common purposes.
Mass protest and grassroots community organization can work together.
When public protests and other forms of disruption increase, so do the grassroots organizations that address prevailing issues. For example, protests regarding pro-life (anti-abortion) interests were associated with increases in local organizations supporting this and other related causes. When public concern declines, so does organizing at the grassroots. Although protest nourishes organization, the reverse does not hold. Organization doesn’t produce protest — it may even retard it (as when agencies may avoid controversy to protect their funding).
Community organizations form when people are ready to be organized.
Although organizations may exist to promote interest in an issue, such as child hunger, little will happen until a significant number of people care about the issue and feel that their actions can make a difference. A big challenge is figuring out when your issue matters to enough people who share a common place or experience, so they can be organized around the issue.
Institutions that want to avoid conflict and controversy may be a difficult base for community organization work.
Consider the case of a school-community initiative to prevent adolescent pregnancy or HIV/AIDS. Although schools are well positioned to deliver information and health services to youth, school officials often oppose providing sexuality education or enhanced access to contraceptives for those who choose to be sexually active. So, human service agencies and educational institutions that rely on public funding may be bad choices for lead agencies in community organization efforts that are likely to draw opposition.
COMMUNITY PLANNING
Societal and community problems are evidence that institutions are not functioning for people.
Much of the framing of societal problems in the 1980s and 1990s focused on the personal attributes of those immediately affected. For example, stated “causes” of high rates of youth crime may highlight the values and behavior of youth and their families such as “poor anger control” or “bad parenting.” Such analyses rarely emphasize the contribution of broader environmental conditions, such as availability of jobs or chronic stresses associated with low income, and the institutions responsible for them. In addition to individual responsibility, public institutions — such as schools, business, religious organizations, and government — should be held accountable for widespread problems in living.
It’s essential to set realistic goals for community organization efforts.
Community-based initiatives often overpromise, particularly with grantmakers. Setting unrealistic objectives — for example, to reduce academic (school) failure by 50 percent in the next two years — sets the group up for perceived failure. Organizations should carefully assess the feasibility of their proposed aims.
If we set only modest goals, we will probably achieve less.
Although goals ought to be achievable, they should also be challenging. Objectives can be overly modest. For example, an overly modest goal might be to reduce rates of school failure (now at 80 percent) by 10 percent within three years. Insufficiently challenging objectives may not bring forth the necessary effort, resources, and degree of change needed to address the community’s concern.
Social planning can engage experts (and local people) in helping address societal problems, particularly when there is consensus on the issue.
We can advance locally valued purposes by engaging technical experts and local people in defining problems and solutions. Outside experts, such as university-based researchers or public officials, can assist local people in obtaining and interpreting data, facilitating the process of setting priorities, and identifying promising alternatives. But planning can go beyond the traditional roles of facilitating coordination and communication among agencies to identifying environmental conditions to be changed.
Locality development or self-help efforts can also assist in addressing community issues.
Local people have the experiential knowledge to come together to define local issues, such as neighborhood safety or jobs, and take action in addressing them. Such self -help efforts have their roots in the settlement house movement in urban neighborhoods. They are guided by respect for the autonomy of local people to decide (and act on ) what matters to them.
Local control can hinder collaboration at broader levels of planning.
Planning at higher levels than the neighborhood, city, or town may be necessary to address the broader conditions that affect community organization efforts. For example, the growing concentration of poverty in the urban core, a result of regional planning decisions and other broader policies, is a structural issue that affects community development efforts within inner-city neighborhoods. Although it’s desirable for community building, strong local control may hinder the broader planning and coordination necessary to address local issues.
COMMUNITY ACTION AND MOBILIZATION
Each individual has the capacity for self-determination, self-help, and improvement.
A basic assumption of community organization is that people most affected by local concerns, including those labeled as “clients” of agency services, can do something about them. This “strengths” perspective highlights people’s assets and abilities, not their deficits and limitations. While it acknowledges personal and community competence, it also recognizes the importance of environmental supports and barriers that affect engagement in community life. For self-determination efforts to be successful, we must create opportunities for working together, and increase the positive consequences of community action.
You can’t do it by yourself.
Addressing what matters to local people — good health, education, and jobs, for example — is beyond any one of us. The idea of “ecology” — interactions among organisms and the environment — helps us see community action as occurring within a web of relationships. Community life is enhanced when individual strengths are joined in common purpose — an expression of the principle of interdependence. We are interconnected: each of us has a responsibility to make this a world good for all of us.
Strong leaders are present in even the most economically deprived communities.
Authentic leaders — those who enable constituents to see higher possibilities, and pursue them together — are among us. Yet, they may not always be acknowledged by those in authority. When doing community organizing in low-income public housing, I found that a simple question helped in “discovering” local leaders: “Who do children go to when they are hurt and an adult isn’t home?” Such questions help us discover the “servant leaders” among us: those who “lead” by addressing the interests of their “followers.”
Community practitioners should never get used to the terrible conditions they see in their community work.
Those doing community work, particularly in low-income communities, are exposed to horrible things: children in uncaring and unhealthy environments; adults without adequate food, clothing, and shelter; and other conditions essential for a decent life. Practitioners should avoid becoming desensitized about how they feel about what they see and hear. Disclosing experiences and feelings to colleagues is one way to help support each other. Community activists must also decide how to use those feelings — such as anger about conditions in which some people live — to energize and sustain their work.
People’s beliefs and values enable them to stay committed.
To make a difference, those doing community work must be in it for the long haul. People’s values, such as fairness or respect for the dignity of others, help sustain their efforts. For instance, a personal or family history of discrimination — a common experience for many racial and ethnic minorities — may incline us to embrace the value of social justice and to work for equality of opportunity.
The work of community organization is like that of a “secular church.”
Faith communities and religious institutions help shape our beliefs about what is right and good, such as our responsibility to care for others. Community-based organizations, such as a homeless coalition or tenants-rights organization, call us to serve the common good — things beyond ourselves. As such, they enable us to devote our lives to higher purposes, while working in this world.
Community practitioners have few opportunities to reflect on the work.
Those doing the work of community building are often consumed by its demands. For example, leaders and staff of community-based organizations rarely take time to consider the lessons learned about community action, barriers and resources, or other features of their work. Personal reflection journals and periodic group retreats help leaders and groups to reflect on and review the initial purposes and recent directions of their organizations. As such, they promote “praxis” — the joining of understanding (theory) and action (practice).
Responding to events and opportunities to build community often takes us beyond what we know.
Community practice is largely an art form. Effective intervention is shaped more by trial and error than by tested general statements about the conditions under which specified interventions (the independent variable) effect desired behavior and outcome (the dependent variables). Yet, attention to the conditions that matter to local people — crime, drug use, and poverty, for example — cannot wait for the findings of research trials. We must be decisive in the face of uncertainty, even when the scientific evidence for a chosen course of action is inadequate.
UNDERSTANDING (AND ADDRESSING) OPPOSITION AND RESISTANCE
Societal problems sometime serve the interests of those in power.
For example, a regulatory policy that permits environmental polluters to go unpunished serves the economic interests of businesses that pollute, and those elected and appointed officials who may benefit from campaign contributions or bribes. Similarly, the existence of drugs and violence may indirectly benefit elected officials since they often gain public support when they rant against perpetrators of drugs and violence. When those in authority oppose community action efforts (or ignore appeals for substantive intervention), there may be a disconnect between the public interest (common good) and the private interests of those with disproportionate influence.
Racial and ethnic tension and controversies have disrupted and destroyed many community organization efforts.
Race and ethnic differences matter in this work. For instance, most African Americans share a common history of discrimination based on race, such as being followed more closely in a store or being ignored by cabs in a city. When you are part of an ethnic minority, people may assume they can think and speak for you, even if they have given no evidence that they care about you. Accordingly, understandable distrust of the “other” (the majority culture) may breed conflict that disrupts reciprocity and collaboration among people of different races and cultures.
Social action tactics, such as disruptive protest, have many detractors.
Participating in (or supporting) protest can be dangerous, especially for those who remain in the community. For example, following a school boycott launched by residents of a low-income public housing project, it was my friend Myrtle Carter, a welfare mother and visible leader, who was subjected to police harassment. She was arrested and jailed for a minor parking violation while we outside organizers who were also part of the effort experienced only small inconveniences. Activists using protest tactics should expect those in power to retaliate, even by establishing criminal penalties for particularly effective disruptive actions such as strikes.
Less in-your-face social action approaches can produce a strong political base from which to make change.
For example, the Industrial Areas Foundation (IAF) appeared to be relatively effective in attracting support (and avoiding opposition) for their causes. Consistent with the “I Ching” and other statements of Eastern philosophies, less direct or forceful actions may be less likely to beget opposition and adverse reaction.
Opposition and resistance may come in many forms.
An analysis of the advocacy literature suggests different ways in which change efforts might be blunted. These include deflecting attention from the issue, delaying a response, denying the problem or request, discounting the problem or the group, deceiving the public, dividing and conquering the organization, appeasing leadership with short-term gains, discrediting group members, or destroying the group with slur campaigns through the media. Skilled practitioners can help group members recognize (and avoid or counteract) sources and modes of opposition.
Community organizations may respond to opposition with appropriate counteractions.
Consider the case of local welfare officials (the opposition) who discount claims of a disability rights group that people with disabilities are being denied assistance unfairly. To counteract this opposition, disability advocates might document the number and kinds of cases denied, and use media advocacy about the consequences of denying eligibility to arouse public concern. Depending on the nature and form of opposition, appropriate counteractions may include reframing the issues, turning negatives into positives, going public with opponents’ tactics, concentrating the organization’s strength against the opponents’ weakness, and knowing when to negotiate.
Opposition to change may be like an onion.
Advocates should expect multiple layers of opposition and resistance to community and system change. For example, community organizations working for better schools may face resistance initially from school board officials; later, from local principals; and still later, from teachers. Peel off one layer, and another form of resistance or opposition may be there to protect vested interests.
INTERVENTION AND MAINTENANCE OF EFFORTS
The strategy of community organization should fit the situation.
The broad and specific means of intervention should match the ends, and the context. For example, social planning — using technical information often with the guidance of outside experts — may assist in defining goals when people share common interests. Similarly, locality development — featuring self-help efforts of local people — may be appropriate for reducing a particular problem, such as substance use or neighborhood safety, around which there is widespread agreement. In contrast, social action — with its disruptive tactics and related conflict — may be needed in contexts of opposing interests such as in reducing discrimination or disparities in income or power.
Using multiple strategies usually has an advantage over any single strategy.
Some initiatives — for instance, a campaign for school reform — get stuck using one preferred means of action, such as collaborative planning or disruptive tactics, even when the goals or conditions shift. By invoking only one strategy, the organization’s actions may be easier to ignore and the benefits of complementary approaches may go untapped. For example, the threat of disruptive tactics (social action) may make support for self-help efforts (locality development) more likely. Flexibility in strategy, and use of multiple means, may enhance community efforts and outcomes.
Being in two cultures promotes creativity.
Some community practitioners operate in more than one system of influence. For example, those who combine research and practice must respect the influences of both academic disciplines and members of community-based organizations. Being open to different audiences helps integrate disparate ideas, discover novel solutions, and transform practice.
The work of community organization takes time, and follow-through.
Mobilizing people for action requires substantial time and effort. Making the calls and personal contacts to bring about a change in school policy, for example, cannot be done solely by volunteers. The stimulation and coordination of community work, like any other valued work, should be paid for. Without salaries for community mobilizers or organizers, follow-through on planned actions is rare.
External support may be both a necessity and a trap for community organizations.
Community organization efforts seldom are maintained without external resources.Yet, financial support usually has strings attached. For example, accepting money from foundations or the government may restrict advocacy efforts. Although often a necessity, outside resources may come at the price of compromising the group’s goals or available means of action.
Community organizations often fade away.
When the issue that a community organization was formed around begins to fade, so may the organization. For example, a taxpayer rights organization may dissolve when its goal of blocking a particular public expenditure, such as a school bond issue, is resolved. Organizations that endure after the issue subsides may lose members unless they reinvent themselves to address other emerging issues.
Organizations need small wins.
“Small wins” are shorter-term, controllable opportunities that can make a tangible difference. For example, a good neighborhood organizer might work for improved trash pickup or more streetlights to provide (literally) visible benefits of group action. Without the small victories, community organizations won’t retain current members — or attract new ones.
PROMOTING COMMUNITY CHANGE
The central ideal of community organization practice is service.
Practitioners’ interests should always be lower on the list than the interests of those of the people served. Yet, when disciplines, such as social welfare or public health, market training for “professionals” in the work of community organization, they risk creating professions in which the practitioners benefit more than the clients. Professions that certify people — and not promising practices or demonstrably effective methods — may emphasize the interests of professionals (or guild interests), and not those experiencing the problems.
Community organization must go beyond the process of bringing people together.
For some practitioners, dialogue among representatives of different groups is a sufficient “outcome” of community development efforts. Yet, local people who come together to address what matters to them are usually interested in going beyond talk, and on to action and achieving results. Community organization efforts should bring about tangible benefits such as community change, problem solving, and furthering social justice.
The primary need is not for individuals to adjust to their world, but for environments to change so people can attain their goals.
Much framing of societal problems focuses on the deficits of those most affected. For example, prominent labels for causes of academic failure might include “poor motivation” (of youth) or “poor monitoring” (by parents). Alternatively, analyses of academic failure might address such environmental conditions as “few opportunities to do academic work” (in schools) and “limited opportunities for employment” (following school). Community health and well being are private and public matters, calling for both individual and social responsibility.
Community-based organizations can function as catalysts for change.
Effective community organizations transform the environment: they alter programs, policies, and practices related to the group’s mission. For example, a disability rights organization might modify policies regarding employment discrimination against people with disabilities or establish new job training programs that accommodate people with different impairments. In their role as catalysts for change, community organizations convene others, broker relationships, and leverage resources for shared purposes.
INFLUENCING SYSTEMS (OR BROADER) CHANGE
The level(s) of intervention should reflect the multiple levels that contribute to the problem.
Consider the typical interventions for most societal problems. For example, job training to address unemployment or drug awareness programs to counter substance use, is typical of initiatives trying to change the behavior of those with limited power who are closest to the “problem,” for instance, low-income adults (unemployment) or youth (substance use).
When used alone, service programs and targeted interventions, such as for so-called “at risk” adults or youth, may deflect attention away from more root causes, such as poverty and the conditions of opportunity that affect behavior at a variety of levels. Resolution of many societal issues, such as crime or unemployment, requires changes in decisions made by corporate and political decisionmakers at levels higher than the local community.
Systems change does not occur simply by reporting felt needs to appointed or elected officials.
For those with higher economic or political status, simply expressing a concern may have influence on decisions that affect them. A variety of traditional means is available to such groups as a way of exerting influence; they include petitioning, lobbying, influencing the media, supporting political candidates, and voting in large numbers. These means are largely unavailable to those most affected by many societal problems, however, such as children and the poor. Marginalized groups lack the resources to exert influence in conventional ways.
The great power of social movements is in communicating a different vision of the world.
Marginalized groups use the drama of protest — and the conflict it provokes — to display realities not widely regarded as important. For example, the media may cover a strike and related protests by farm workers or coal miners, and the violence it often evokes from owners, the police, or others in power. Media coverage helps convey the story of the conditions faced by the protesters, and the unfairness of the action (or inaction) of businesses or institutions that are targeted. The dramatic nature of protest and related conflict can help politicize voters who, through enhanced public support of the positions of marginalized groups, can exert influence on those in power.
Community organizations should seek changes within their power to manage.
Since ignoring is likely and retaliation is possible, small organizations with limited power should avoid seeking fundamental changes in the system. For example, a single grassroots organization in a low-income neighborhood may not be positioned to effect systems changes such as altering the priorities of grantmakers who support work in the community. But, small and scrappy organizations may succeed in bringing about community change when their bulkier counterparts do not.
Community and broader systems change can be brought about through collaboration.
Collaboration involves alliances among groups that share risks, resources, and responsibilities to achieve their common interests. For example, local community-based organizations interested in the well being of children can link with each other to create local programs (e.g., mentoring), policies (e.g., flextime to be with children after school) and practices (e.g., adults caring for children not their own).
Additionally, broader partnerships with grantmakers, government agencies, and business councils can affect the conditions in which change occurs at the community level. An example is altering grantmaking programs to support collaborative work or promoting child-friendly business policies through industrial revenue bonds or new corporate policies. Collaborative partnerships help bring about community and system change when they link local people to resources and institutions at the multiple levels in which change should occur to address common interests.
ACHIEVING COMMUNITY-LEVEL IMPROVEMENTS
Societal problems often reoccur.
Consider the problem of gang violence that occurred after World War II and reoccurred in the 1990s. Broad social conditions — wide disparity of income, weak social ties, and related mistrust of others — appear to affect the likelihood of societal problems such as increased death rates, infant mortality, and perhaps youth violence. Improvements achieved in one era may need to be reestablished by future generations that must again transform the environmental conditions that support the reoccurrence of societal problems.
Most community efforts “chip” away at the problem.
The majority of community interventions do not match the scale of the problem. For example, a community effort may prepare 10 unemployed people to compete for only one available job, or may create 100 jobs in a community with thousands of unemployed. We often make small changes in a context that remains unchanged.
Real change is rare.
Significant improvements in community-level outcomes are highly unusual — such as cases of reducing rates of adolescent pregnancy or academic failure by 50 percent or more. Yet, in requests for grants, community-based organizations often promise (and grantmakers expect) statements of objectives that indicate significant improvements as a result of only modest investments over a short time. We should not perpetuate myths about what most interventions can actually accomplish.
Development of community leadership may be a positive byproduct of even a “failed” community effort.
Although an initiative may not produce statistically significant changes in community benchmarks or indicators, it may develop new leaders or build capacity to address new issues in the future. For instance, a public health initiative that produces only modest reductions in rates of adolescent pregnancy may develop the capacity to produce changes that matter, such as four years later when the group switches its efforts from adolescent pregnancy to child well-being.
Community documentation and evaluation must help us see what is actually achieved by community initiatives, including evidence of intermediate outcomes (e.g., community and system change) and other indicators of success or “failure” (i.e., community capacity over time and across issues).
Optimal health and development for all people may be beyond the capacity of what communities can achieve, but not beyond what they should seek.
Most community-based efforts, such as those to create healthy environments for all our children, will fall short of their objectives. Yet, justice requires that we create conditions in which all people can make the most of their inherently unequal endowments. Support for community initiatives should be guided by what we must do for current and future generations, not by what limited gains we have made in the past.
IN SUMMARY
The fundamental purpose of community organization — to help discover and enable people’s shared goals — is informed by values, knowledge, and experience. This section outlined lessons learned from the experiences of an earlier generation of community organization practitioners (each with an average of over 40 years of experience). The insights were organized under broad themes of community organization practice.
Community organization often has a bottom-up or grassroots quality: people with relatively little power coming together at the local level to address issues that matter to them. For example, grassroots efforts may involve planning by members of a neighborhood association, protests by a tenants’ organization, or self-help efforts of low-income families to build local housing.
Yet, community organization may also function as a top-down strategy, such as when elected or appointed officials — or others in power — join allies in advancing policies or resource allocations that serve their interests. Bottom-up and top-down approaches to community organization may work in conflict, such as when appointed officials conspire to make voter registration of emerging minority groups more difficult. Top-down and bottom-up efforts may also work in concert, as when grassroots mobilization, such as letter writing or public demonstrations, help support policy changes advanced by cooperative elected or appointed officials working at broader levels.
Community organization strategies may be used to serve — or hinder — the values and aims of particular interest groups. Consider the issue of abortion: those organizing under the pro-choice banner may use protest tactics to advance policies and practices that further individual freedom (a woman’s “right” to choose whether to have an abortion). Alternatively, those working on the pro-life side may organize to seek changes consistent with the value of security and survival (an unborn child’s “right” to life). Depending on our values and interests, we may support or denounce the use of similar disruptive tactics by proponents or opponents of the issue.
What is the relationship between personal values and qualities — and the experiences and environments that shaped them — and the work of community organization and change? Personal background, such as a basic spirituality or a history of discrimination associated with ethnic minority status, can predispose a practitioner to support particular values, such as social justice or equality, consistent with the work of community organization.
What qualities and behaviors of community organizers, such as respect for others and willingness to listen, help bring people together? Many of these attributes and behaviors — including clarity of vision, capacity to support and encourage, and tolerance of ambiguity — are similar to those of other leaders.
How do we cultivate such natural leaders, and nurture and support their work in bringing people together? Further research may help clarify the relationship between personal qualities and behaviors, such as those of the “servant” or “servant leader ,” the broader environment that nurtures or hinders them, and the outcomes of community organization efforts.
Finally, leadership in community work may begin with a few good questions:
- What is desired now, in this place, by these people?
- What is success?
- Under what conditions is improvement possible?
- How can we establish and sustain conditions for effective community problem solving? over time, and across concerns?
- How would we know it?
Imagine a “living democracy” — large numbers of people, in many different communities, engaged in dialogue about shared concerns and collective action toward improvement. Perhaps these lessons — inspired by reflections of an earlier generation of community organization practitioners — can help us better understand and improve the essential work of democracy: people coming together to address issues that matter to them.
Online Resources
Chapter 5: Theories in the “Introduction to Community Psychology” explains the role of theory in Community Psychology, the main foundational theories in the field, and how community psychologists use theory in their work.
Chapter 15: Community Organizing, Partnerships, and Coalitions in the “Introduction to Community Psychology” describes how and why communities organize, bottom-up and top-down approaches to community organizing, and the cycle of organizing.
Theory In Community Organization: People Have the Power! is a downloadable PowerPoint presentation that elaborates about theory in community organization.
Print Resources
Adler, M. (1981). Six great ideas: truth, goodness, beauty, liberty, equality, justice: ideas we judge by, ideas we act on. New York, NY: Macmillan.
Alinsky, S. (1969). Reveille for radicals. Chicago: University of Chicago Press.
Altman, D., Balcazar, F., Fawcett, S. B., Seekins, T., & Young, J. (1994 ). Public health advocacy: Creating community change to improve health. Palo Alto, CA: Stanford Center for Research in Disease Prevention.
Balcazar, F., Seekins, T., Fawcett, S., & Hopkins, B. (1990). Empowering people with physical disabilities through advocacy skills train. American Journal of Community Psychology, 18, 281-295.
Bracht, N. (Ed.) (1990). Health promotion at the community level. Newbury Park, CA: Sage Publications.
Brager, G. & Specht, H. (1973). Community organizing. New York, NY: Columbia University Press.
Branch, T. (1988). Parting the waters: America in the King years 1954-63. New York, NY: Simon and Schuster.
Brown, M. (2006). Building powerful community organizations: A personal guide to creating groups that can solve problems and change the world. Arlington, MA: Long Haul Press.
Cobb, R., & Elder, C. (1972). Participation in American politics: The dynamics of agenda-building. Baltimore: The Johns Hopkins University Press.
Cook, T. & Campbell, D. (1979). Quasi-experimentation: Design and analysis issues for field settings. Chicago: Rand McNally.
Cox, F., Erlich, J., Rothman, J., & Tropman, J. (1987). Strategies of community organization: Macro practice. (4th ed.). Itasca, IL: F. E. Peacock Publishers, Inc.
Cuoto, R. (1990). Promoting health at the grass roots. Health Affairs, 9, 145-151.
Dass, R. & Gorman, P. (1985). How can I help? Stories and reflections on service. New York, NY: Alfred A. Knopf.
Dunham, A. (1963). Some principles of community development. International Review of Community Development, 11, 141-151.
Fawcett, S. (1991). Some values guiding community research and action. Journal of Applied Behavior Analysis, 24, 621-636.
Fawcett, S., Lewis, R., Paine, A., Francisco, V., Richter, K., Williams, E., & Copple, B. Evaluating community coalitions for the prevention of substance abuse: The case of Project Freedom. Health Education and Behavior.
Fawcett, S., Paine, A., Francisco, V., Vliet, M. (1993). Promoting health through community development. Promoting Health and Mental Health in Children, Youth, and Families (pp. 233-255). D. S. Glenwick & L. A. Jason (Eds.). New York, NY: Springer Publishing Company.
Fawcett, S., Paine, A., Francisco, V., Schultz, J., Richter, K., Lewis, R., Williams, E., Harris, K., Berkley, J., Fisher, J., & Lopez, C. (1995). Using empowerment theory in collaborative partnerships for community health and development. American Journal of Community Psychology, 23, 677 -697.
Fawcett, S., Paine, A., Francisco, V., Schultz, J., Richter, K., Berkley, J., Patton, J., Fisher, J., Lewis, R., Lopez, C., Russos, S., Williams, E., Harris, K., & Evensen, P. Evaluating community initiatives for health and development. In I. Rootman, D. McQueen, et al. (Eds.) Evaluating health promotion approaches. Copenhagen, Denmark: World Health Organization – Europe.
Fawcett, S., Seekins, T., & Silber, L. (1988). Low-income voter registration: A small-scale evaluation of an agency-based registration strategy. American Journal of Community Psychology, 16, 751-758.
Fawcett, S. (1999). Some lessons on community organization and change. In J. Rothman (Ed.). Reflections on Community Organization: Enduring Themes and Critical Issues. Itasca, Illinois: F. E. Peacock Publishers.
Fisher, R. (1987). Community organizing in historical perspective: A typology. In F. M. Cox, J. L. Erlich, J. Rothman, and J. E. Tropman. (pp. 387-397). Strategies of Community Intervention: Macro Practice. (4th ed.). Itasca, IL: F. E. Peacock Publishers, Inc.
Gardner, J. (1990) On leadership. New York, NY: Free Press.
Gaventa, J. (1980). Power and powerlessness: Quiescence and rebellion in an Appalachian valley. Chicago: University of Illinois Press.
Greenleaf, R. (1997). Servant leadership. New York, NY: Paulist Press.
Heifetz, R. (1994). Leadership without easy answers. Cambridge, MA: Belnap Press of Harvard University Press.
Himmelman, A. (1992). Communities working collaboratively for a change. (Monograph available from the author, 1406 West Lake, Suite 209, Minneapolis, MN 55408)
Jargowsky, P. (1997). Poverty and place: Ghettos, barrios, and the American city. New York, NY: Russell Sage Foundation.
Kingdon, J. (1995). (2nd Ed.). Agendas, alternatives, and public policies. Boston: Little, Brown.
Lappe, F. & Dubois, P. (1994). The quickening of America. San Francisco: Jossey-Bass.
Mathews, R.. & Fawcett, S. (1984). Building the capacities of job candidates through behavioral instruction. Journal of Community Psychology, 12, 123 -129.
Morris, A.. (1984). The origins of the civil rights movement. New York, NY: The Free Press.
Newstetter, W. (1947). The social intergroup work process. In Proceedings of the National Conference of Social Work. (pp. 205-217). New York, NY: Columbia University Press.
Paine, A., Francisco, V., & Fawcett, S. (1994). Assessing community health concerns and implementing a microgrants program for self-help initiatives. American Journal of Public Health, 84(2), 316-318.
Paine, A., Fawcett, S., Richter, K., Berkley J., Williams, E., & Lopez, C. Community coalitions to prevent adolescent substance abuse: The case of the “Project Freedom” replication initiative. Journal of Prevention and Intervention in the Community.
Paine, A., Harris, K., Fawcett, S., Richter, K., Lewis, R., Francisco, V., Johnston, J., Coen, S. Evaluating a statewide partnership for reducing risks for chronic diseases. Journal of Community Health.
Paine, A., Vincent, M., Fawcett, S., Campuzano, M., Harris, K., Lewis, R., Williams, E., & Fisher, J. (1996). Replicating a community initiative for preventing adolescent pregnancy: From South Carolina to Kansas. Family and Community Health, 19(1), 14-30.
Perlman, R. & Gurin, A. (1972). Community organization and social planning. New York, NY: John Wiley.
Piven, F. & Cloward, R. (1977). Poor people’s movements: Why they succeed, how they fail. New York, NY Random House.
Rappaport, J., Swift, C., & Hess, R. (Eds.). (1984). Studies in empowerment: Steps toward understanding and action. New York, NY: Haworth.
Ross, M. (1955). Community organization: Theory and principles. New York, NY: Harper and Brothers.
Rothman, J. (Ed.). (1999). Reflections on community organization: Enduring themes and critical issues. Itasca, Illinois: F.E. Peacock Publishers.
Rothman, J., & Tropman, J. (1987). Models of community organization and macro practice perspectives: Their mixing and phasing. In Cox, F., Erlich, J., Rothman, J., & Tropman, E. (Eds.), Strategies of community organization: Macro practice (4th ed.) (pp. 3-26). Itasca, IL: F.E. Peacock Publishers.
Schriner, K., Fawcett, S. (1988). A community concerns method for local agenda setting. Journal of the Community Development Society, 19, 108-118.
Seekins, T. & Fawcett, S. (1987). Effects of a poverty clients’ agenda on resource allocations by community decisionmakers. American Journal of Community Psychology, 15, 305-320.
Seekins, T., Maynard, S., & Fawcett, S. (1987). Understanding the policy process: Preventing and coping with community problems. Prevention in Human Services, 5 (2), 65-89.
Stull, D., & Schensul, J. (1987). Collaborative research and social change: Applied anthropology in action. Boulder, CO: Westview.
Suarez de Balcazar, Y., Bradford, B., & Fawcett, S. (1988). Common concerns of disabled Americans: Issues and options. Social Policy, 19 (2), 29-35.
Tax, S. (1952). Action anthropology. American Indigena, 12, 103-106.
Watzlawick, P., Weakland, J. H., & Fisch, R. (1974). Change: Principles of problem formation and problem resolution. New York, NY: Norton.
Weick, K. E. (1984). Small wins: Redefining the scale of social problems. American Psychologist, 39, 40-49.
Wilkinson, R. G. (1996). Unhealthy societies: The afflictions of inequality. London: Routledge.
World Health Organization. (1986). The Ottawa charter for health promotion. Health Promotion, 1, iii-v.
Yin, R. (1988). Case study research: Design and methods. Newbury Park, CA: Sage.
Zald, M. (1987). Organizations: Organizations as polities: An analysis of community organization agencies. In Cox, F., Erlich, J., Rothman, J., & Tropman, E. (pp. 243-254). Strategies of community organization: Macro practice. (4th ed.). Itasca, IL: F. E. Peacock Publishers, Inc.
